

A Master’s-Level Case Study of NHS England Older People’s Care and Buurtzorg-Inspired Community Support
Research Publication by Juliet C. Nwaiwu
Institutional Affiliation: New York Center for Advanced Research (NYCAR)
Publication No.: NYCAR-TTR-2026-RP026
DOI: https://doi.org/10.5281/zenodo.20449332
Date: June 2026
Peer Review Statement
This research publication has been reviewed under the internal editorial framework of the New York Center for Advanced Research (NYCAR) and The Thinkers’ Review. The review assessed master’s-level coherence, gerontological source integrity, NHS England and Buurtzorg case suitability, quality-of-life reasoning, quantitative-model suitability, APA 7th alignment, safeguarding sensitivity, and professional relevance for ageing-care leadership. The work is approved for master’s-level NYCAR institutional publication.
Copyright © June 2026 Juliet C. Nwaiwu. All rights reserved. NYCAR.
Contents
Gerontological Care Leadership and Quality of Life in Aging Societies
A Master’s-Level Case Study of NHS England Older People’s Care and Buurtzorg-Inspired Community Support
Research Publication by Juliet C. Nwaiwu
Institutional Affiliation: New York Center for Advanced Research (NYCAR)
Publication No.: To be assigned
DOI: Not assigned
Date: June 2026
Peer Review Statement
This research publication has been reviewed under the internal editorial framework of the New York Center for Advanced Research (NYCAR) and The Thinkers’ Review. The review assessed master’s-level coherence, gerontological source integrity, NHS England and Buurtzorg case suitability, quality-of-life reasoning, quantitative-model suitability, APA 7th alignment, safeguarding sensitivity, and professional relevance for ageing-care leadership. The work is approved for master’s-level NYCAR institutional publication.
Copyright © June 2026 Juliet C. Nwaiwu. All rights reserved. NYCAR.
Contents
Abstract 3
Chapter 1: Introduction: Ageing as a Leadership Test 5
Chapter 2: Evidence Base and Conceptual Frame 9
Chapter 3: Methodology and Applied Measurement Design 13
Chapter 4: NHS England Case Analysis: Frailty, Recovery, and System Coordination 18
Chapter 5: Buurtzorg-Inspired Community Support and Relational Continuity 22
Chapter 6: Quantitative Model and Scenario-Based Findings 26
Chapter 7: Leadership Practice, Carer Reality, and Dignity-Centred Implementation 31
Chapter 8: Applied Care Scenarios: Dementia, Falls, Medicines, Housing, and Loneliness 36
Chapter 9: Board Assurance, Commissioning, and Local Implementation 40
Chapter 10: Recommendations and Final Position 45
Appendix A: Measurement Assurance and Local Data Rules 51
References 56
Abstract
Population ageing is often described through pressure: pressure on hospitals, pressure on adult social care, pressure on public finance, pressure on family carers. That language is not false, but it is incomplete. Longer life is also a social achievement, and the measure of a mature care system is whether added years are lived with safety, purpose, connection, and practical help. Older people do not experience care as a service map. They experience it in the stair they cannot climb, the tablet they cannot identify, the staff member they do not recognize, the daughter who is exhausted, the appointment that arrives too late, and the evening when loneliness becomes fear.
This master’s-level study examines gerontological care leadership and quality of life through two connected case lenses: NHS England older people’s care and Buurtzorg-inspired community support. NHS England’s public evidence shows the importance of integrated pathways, urgent community response, frailty care, discharge support, reablement, and short-term intensive support outside hospital where safe. Buurtzorg-derived practice adds a different lesson: relational continuity, professional discretion, small-team accountability, and the value of knowing the person’s home life rather than treating care as a chain of brief tasks.
The paper uses public evidence from NHS England, Age UK, the Care Quality Commission, the Office for National Statistics, the Centre for Ageing Better, the World Health Organization, Skills for Care, and peer-reviewed research on integrated care, Buurtzorg-derived models, self-managing teams, multimorbidity, virtual wards, and home-care supply. Quantitative reasoning is applied through a quality-of-life score, care-continuity index, dependency ratio, readmission-risk score, service-access time, and an integrated gerontological leadership index. These measures are presented as management tools, not as private NHS or Buurtzorg data.
The central argument is direct: gerontological leadership is credible only when it protects the lived conditions of ageing. A system that moves older people quickly but leaves them unsafe has failed. A system that records many visits but offers no continuity has failed. A system that praises home care while ignoring carers has failed. Quality of life in later life has to be governed as seriously as hospital flow, finance, and activity counts.
Keywords: gerontological care leadership; older people’s care; NHS England; Buurtzorg; quality of life; integrated care; reablement; care continuity; adult social care; ageing societies.
List of Tables and Figures
Table 1. Gerontological care leadership domains
Table 2. Scenario-based measures used in the study
Table 3. NHS England and Buurtzorg-inspired case comparison
Table 4. Implementation assurance questions
Figure 1. Integrated gerontological care leadership model.
Figure 2. Quality-of-life score component weights.
Figure 3. Scenario score profile for gerontological care review.
Figure 4. Case comparison: coordination and relational care.
Figure 5. Implementation cycle for ageing-care leadership.
Chapter 1: Introduction: Ageing as a Leadership Test
Ageing societies are often treated as a demographic problem, as if the growing number of older citizens were itself the crisis. That framing is too narrow. The real test lies in whether health and social care systems can organize timely, respectful, clinically safe, and socially intelligent support around people whose needs rarely fit one professional box. Longer life has been made possible by public health, housing improvements, medical treatment, education, better nutrition, and social protection. Yet a longer life can become painfully small when a person loses mobility, waits too long for help, fears falling, or becomes dependent on strangers who change from visit to visit.
Gerontological care leadership begins with that tension. It does not romanticize ageing, and it does not reduce older people to a burden. It asks how systems can protect function, confidence, dignity, and ordinary life when frailty, multimorbidity, dementia, poverty, housing insecurity, bereavement, and carer strain enter the same home. A person recovering from pneumonia may also live alone, struggle with arthritis, take twelve medicines, hear poorly, and depend on a niece who works full-time. A service that treats each fact separately will miss the person.
England gives this problem a sharp public setting. Age UK has reported persistent pressure in older people’s access to health and care, while the Centre for Ageing Better’s State of Ageing 2025 describes a large and diverse older population in which nearly one in five people in England are aged 65 and over. The Office for National Statistics continues to track population ageing and the growth of the oldest age groups. These are not abstract curves. They shape GP demand, ambulance calls, hospital discharge, home care, safeguarding, rehabilitation, housing adaptation, and the unpaid labour that families provide.
NHS England’s older people’s care examples are relevant because they try to move care closer to the person rather than leaving hospital as the default location for every crisis or recovery period. Short-term intensive support, urgent community response, frailty pathways, virtual wards, and integrated care in action all reveal a policy direction: the person’s own home can be a site of recovery when clinical risk is understood and community support is real. The qualification matters. Home is not safer by definition. Home may be warm, familiar, and supported. It may also be cold, lonely, cluttered, inaccessible, digitally excluded, or held together by a carer who has no reserve left.
Buurtzorg-inspired community support adds another lens because it places relational continuity and professional discretion at the center of home care. The original Dutch model is often discussed with admiration, but imitation is not the point of this study. Small self-managing teams cannot be lifted from one country and installed elsewhere by language alone. Funding rules, labour conditions, regulation, professional boundaries, records systems, safeguarding processes, and local culture determine whether the idea survives practice. Still, the Buurtzorg-derived literature offers an important challenge to task-driven care: older people benefit when professionals know them, know their homes, and can act with judgment rather than only complete a time-limited visit.
This publication treats gerontological care leadership as a management, ethics, and service-quality problem. The manager’s question is not only how many visits were delivered, how many beds were cleared, or how many assessments were completed. The deeper question is whether the service protected what made life livable for the older person: washing, eating, sleeping, moving safely, taking medicines correctly, seeing familiar faces, knowing whom to call, and feeling that decisions were made with rather than around them. Those outcomes are harder to count than throughput, but they are not less real.
The aim of the study is to examine how gerontological care leadership can improve quality of life in ageing societies. It uses NHS England older people’s care and Buurtzorg-inspired community support as applied case evidence, then develops practical indicators for quality of life, continuity, access, demographic pressure, and readmission risk. The publication does not present confidential patient records or private organizational data. It uses public evidence and scenario-based modeling to show how leaders can reason more responsibly about care quality.
The research questions follow from that aim. How does gerontological care leadership shape quality of life for older people? What do NHS England and Buurtzorg-inspired models reveal about integrated care, home-based recovery, continuity, and professional discretion? Which indicators can help managers measure quality without reducing people to scores? How can leaders identify readmission risk, access delay, carer strain, and continuity weakness before they become avoidable harm? What kind of service design protects dignity in later life?
The significance of the study lies in its refusal to treat ageing care as a peripheral concern. Older people’s care is a test of a society’s operational competence and moral seriousness. When the system fails, the consequences appear in emergency departments, delayed discharges, unsafe homes, avoidable admissions, unpaid carer collapse, and lives made smaller than they needed to be. When leadership is capable, the value is often quiet: a fall prevented, a medicine clarified, a daughter reassured, a known nurse arriving on time, a person regaining the confidence to wash and walk again.
Chapter 2: Evidence Base and Conceptual Frame
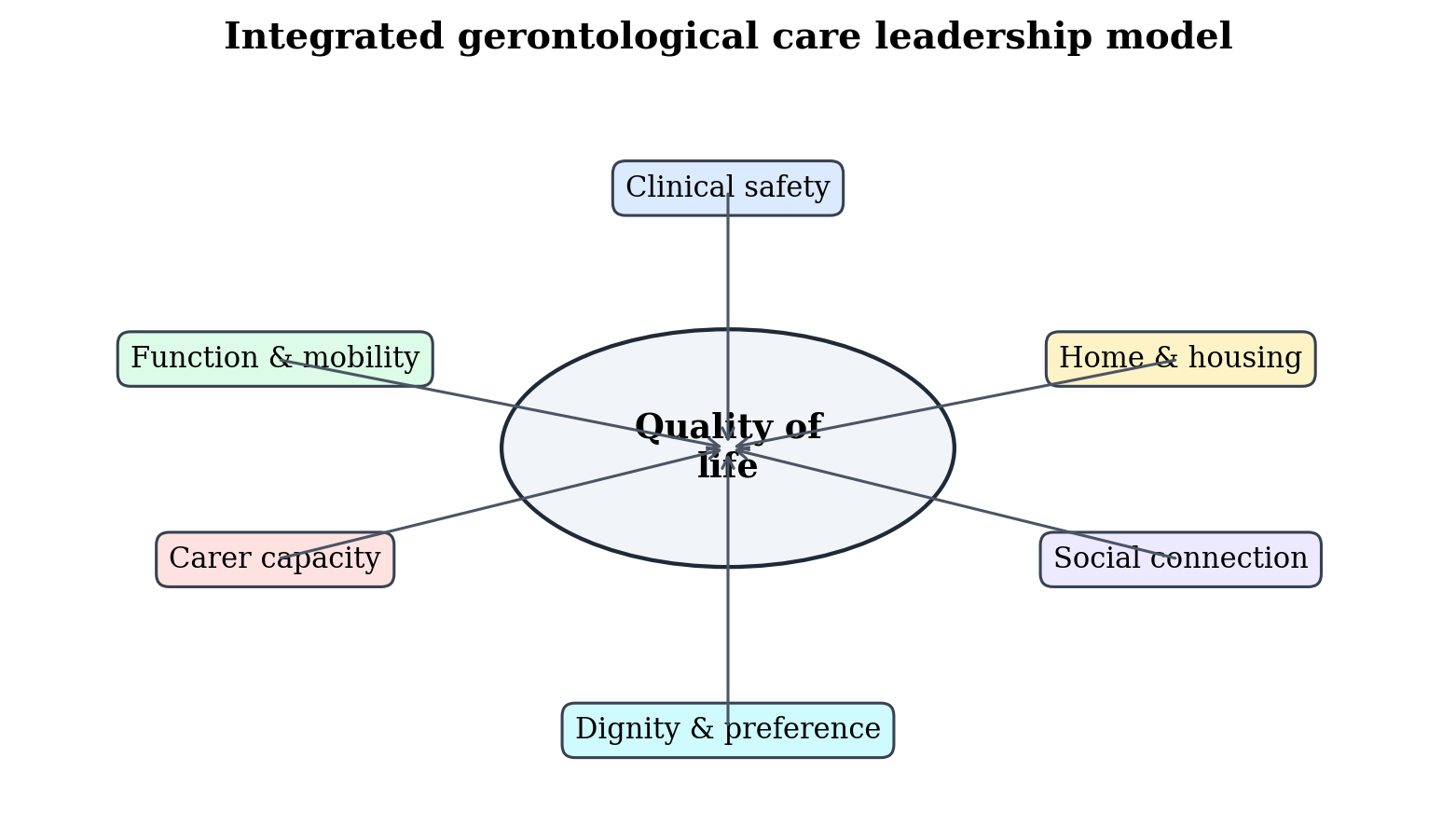
Figure 1. Integrated gerontological care leadership model. Copyright © June 2026 Juliet C. Nwaiwu / NYCAR. All rights reserved.
Gerontology begins with a simple warning: age alone explains very little. Two people of the same age can live radically different lives. One may be working, driving, caring for grandchildren, chairing a local group, and living with mild hypertension. Another may be housebound, bereaved, cognitively impaired, frightened of falling, and dependent on irregular visits. Between those poles lie many combinations of resilience, illness, loss, adaptation, pride, and need. Leadership that treats older people as one administrative category will always be late to reality.
The World Health Organization’s healthy ageing work is useful because it places functional ability at the center of the field. Healthy ageing is not limited to the absence of disease; it concerns the environments and opportunities that allow people to be and do what they value. The WHO ICOPE approach similarly emphasizes person-centred, coordinated care that attends to intrinsic capacity and functional ability across later life. For managers, this shifts the question. The service is not assessed only by diagnosis, activity, or discharge. It is assessed by whether the person can live with meaning, safety, and practical control.
Age UK’s recent reporting gives the English context more urgency. Its 2025 report reviewed a decade of change in older people’s health and care, and the 2024 edition noted that people aged over 50 already made up about two in five of England’s population, with the 85-plus group growing most rapidly. Those facts matter because very old age is often where frailty, dementia, multimorbidity, falls risk, sensory loss, bereavement, and care dependency cluster. Demography alone does not dictate crisis, but poor preparation converts demography into avoidable pressure.
The Care Quality Commission’s 2024/25 State of Care evidence also belongs in the core framework because it links delayed discharge to real capacity gaps. CQC reported that, for people in acute hospital for 14 days or longer in March 2025, lack of social care capacity and delays completing social care transfer plans accounted for 23 percent of delayed discharges, while access to rehabilitation, reablement, and recovery services accounted for 26 percent. These figures put gerontological leadership beyond the hospital ward. Older people cannot recover safely at home if the community layer is too thin to meet them.
Integrated care research makes the same point from another angle. Dambha-Miller, Simpson, Hobson, Chapman, and Damery examined integrated primary care and social services for older adults with multimorbidity in England and found a field marked by varied models, local complexity, and continuing implementation challenges. Multimorbidity does not respect professional boundaries. A person with diabetes, heart failure, arthritis, cognitive impairment, anxiety, and housing risk is not a sequence of problems. The person is one life with several interacting demands.
NHS England’s public case material on older people’s care shows how integrated care can work when it is attached to practical pathways. Its integrated-care-in-action example describes short-term intensive support for up to ten days, including nursing, therapeutic assessment, and social care, designed to help patients regain independence. The value of that example lies in its focus on the recovery bridge. Hospital treatment may stabilize illness, but recovery often depends on therapy, confidence, equipment, personal care, and home context. Without that bridge, a discharge becomes a transfer of risk.
Buurtzorg-derived models contribute a different kind of evidence. Hegedüs, Schürch, and Bischofberger’s scoping review described experiences with Buurtzorg-derived home care outside the Netherlands, while de Bruin, Doodkorte, Sinervo, and Clemens reviewed self-managing teams in elderly care. The findings do not support naive transplantation. They point to implementation conditions: staffing, autonomy, team preparation, supervision, local funding, and the ability to maintain accountability without suffocating discretion. The professional lesson is practical. Relationship-based care can improve the texture of support, but only when teams have the means to act responsibly.
Workforce evidence needs a place in the conceptual frame because care quality is embodied. It arrives through nurses, care workers, therapists, social workers, pharmacists, GPs, voluntary-sector staff, and family carers. Skills for Care’s workforce reporting continues to show recruitment and vacancy pressure in adult social care. A model of dignity that ignores workforce stability is ornamental. Older people experience staffing policy as who arrives, whether they arrive on time, whether they know the person’s routine, and whether they have enough time to do the work with care.
Quality of life provides the unifying concept. A service may be clinically safe and still leave a person lonely. It may be efficient and still leave a carer exhausted. It may reduce hospital days and still fail at medicines, food, washing, mobility, or trust. This study treats quality of life as a management outcome because it can be influenced by leadership decisions: staffing patterns, continuity rules, discharge design, assessment quality, carer support, housing links, volunteer partnerships, and the timing of rehabilitation.
Four concepts organize the analysis. The person is the unit of meaning. The care pathway is the unit of coordination. The home is the unit of lived risk. The local system is the unit of accountability. No single profession owns the whole answer. Leadership appears when these levels are brought into conversation and when the service refuses to hide behind one measure of success.
Read also: Value-Based Commissioning In Social Care Systems
Chapter 3: Methodology and Applied Measurement Design
Table 1. Gerontological care leadership domains
| Domain | Leadership question | Quality-of-life relevance |
| Clinical safety | Is risk recognized early and escalated properly? | Protects health, confidence, and safe recovery. |
| Continuity | Does the person see known staff often enough for trust and recognition? | Supports dementia care, safeguarding, and emotional security. |
| Access time | How long does support take to begin after need is identified? | Reduces deterioration caused by delay. |
| Carer capacity | Is unpaid labour being assessed and supported? | Prevents hidden strain and avoidable crisis. |
| Home environment | Does the home support the plan or undermine it? | Links housing, equipment, falls prevention, and independence. |
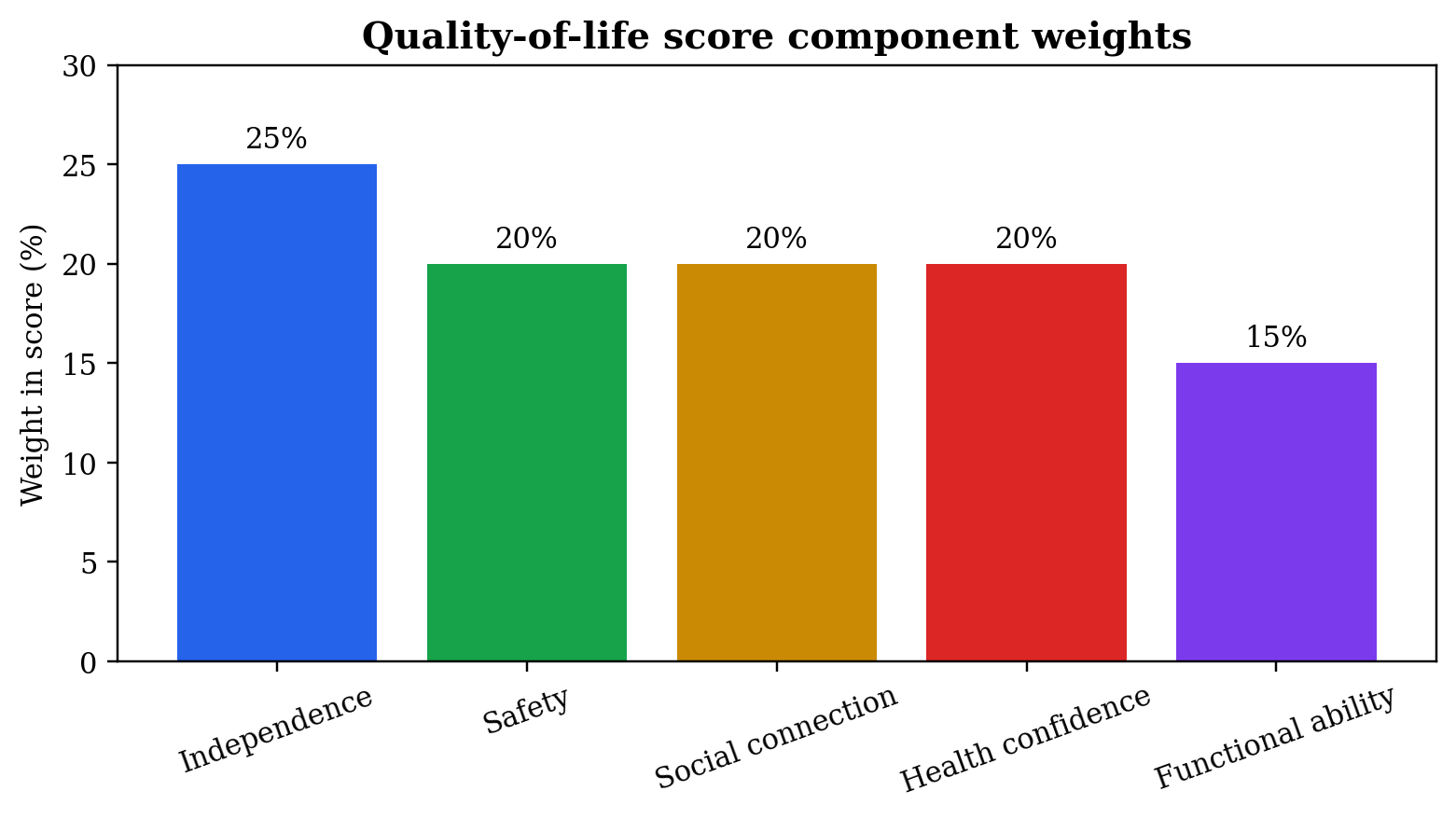
Figure 2. Quality-of-life score component weights. Copyright © June 2026 Juliet C. Nwaiwu / NYCAR. All rights reserved.
This study uses a mixed-methods case-study design. NHS England older people’s care and Buurtzorg-inspired community support are treated as applied cases, while quality of life in ageing societies is the management problem under examination. The qualitative strand reads public documents and research for the way they frame older people’s needs, service coordination, continuity, home-based recovery, and professional responsibility. The quantitative strand develops scenario-based measures for quality of life, care continuity, demographic pressure, readmission risk, access delay, and integrated leadership readiness.
Case selection is purposeful. NHS England older people’s care is selected because it operates within a national health and care system under visible pressure, with public guidance on urgent community response, frailty pathways, proactive care, discharge, integrated care, and home-based support. Buurtzorg-inspired practice is selected because it challenges task-based home care with a model that values self-managing teams, relational knowledge, and professional discretion. The cases are not treated as directly interchangeable. Their value lies in the contrast between system coordination and relationship-centred local practice.
The study uses public evidence only. Sources include NHS England materials, Age UK reports, CQC State of Care reporting, Office for National Statistics population evidence, Centre for Ageing Better analysis, WHO healthy ageing guidance, Skills for Care workforce reporting, and peer-reviewed research on integrated care, home care, Buurtzorg-derived models, self-managing teams, delayed discharge, multimorbidity, and virtual wards. No confidential NHS record, private Buurtzorg file, identifiable patient account, or unpublished local dataset is used.
That boundary matters. Papers on health and social care often lose credibility when they imply access to data they do not possess. This study avoids that error. The measures are not presented as actual NHS performance results or Buurtzorg outcomes. They are management tools that local leaders could adapt with lawful data, patient and carer involvement, and proper governance. The distinction between public evidence, scenario modeling, and local evaluation is maintained throughout the paper.
The primary quality-of-life score is expressed as QoL = 0.25I + 0.20S + 0.20C + 0.20H + 0.15F. I represents independence, S safety, C social connection, H health confidence, and F functional ability. Each component is scored from zero to 100. The weights are illustrative and can be changed after local consultation. A person with dementia, a person recovering from a stroke, and a person living alone after bereavement may rank the components differently. The score is a conversation tool, not a replacement for the person’s account.
The care-continuity index is expressed as CCI = known-team visits / total visits × 100. Continuity has clinical and emotional value. A familiar staff member may notice appetite change, new confusion, unsafe movement, carer strain, or neglected home conditions sooner than a rotating stranger. Yet continuity cannot become rigid protectionism that blocks urgent care. The measure is useful because it shows whether care planning values familiarity enough to measure it.
The dependency ratio is expressed as DR = older population / working-age population × 100. The measure helps local planners think about population structure, workforce demand, carer availability, housing adaptation, transport, and public-health priorities. It requires careful interpretation. Older people are not only users of care; many are workers, volunteers, carers, community leaders, grandparents, and financial contributors. The ratio is a planning signal, not a label of burden.
The readmission-risk score is expressed as RRS = 0.30F + 0.25M + 0.20C + 0.15P + 0.10L. F represents frailty, M multimorbidity, C carer strain, P prior admission history, and L low service access. Higher scores indicate a transition that may require more intensive support after discharge. The ethical rule is clear: risk scoring exists to direct help, not deny it. A high-risk older adult is not a problem to exclude. The score tells the system where responsibility becomes more urgent.
Service-access time is expressed as SAT = average days from identified need to support start. The indicator is simple but serious. Time is not neutral in later life. Waiting for therapy, home care, equipment, continence advice, medication review, or a safeguarding response can change the person’s functional trajectory. A single average can mislead, so access time has to be stratified by urgency, frailty, living arrangement, carer strain, and risk of deterioration.
This study also proposes an Integrated Gerontological Leadership Index, IGLI = 0.20Q + 0.20K + 0.15A + 0.15R + 0.15W + 0.15E. Q represents quality-of-life review, K known-team continuity, A access timeliness, R readmission-prevention practice, W workforce stability, and E equity and carer evidence. Each component is scored from zero to 100. The index is not a league table. It helps a local board ask whether ageing care is being governed as a connected system rather than as disconnected activity.
Validity is protected by making the logic visible. Each measure has a formula, a reason for inclusion, and an ethical caution. The formulas do not make care mechanical. They give leaders a clearer way to discuss what has often been hidden behind good intentions. The score never outranks the older person’s voice. A manager can use a number to open the right conversation, but the meaning of that number requires professional judgment, family context, and local knowledge.
Limitations remain. Public sources cannot show every local failure or every instance of excellent care. Buurtzorg-derived research cannot prove that self-management will work in every setting. Quality of life cannot be fully captured in a formula. The method remains valuable because it translates a broad human problem into a set of accountable management questions.
Chapter 4: NHS England Case Analysis: Frailty, Recovery, and System Coordination
Table 3. NHS England and Buurtzorg-inspired case comparison
| Case lens | Main contribution | Main caution |
| NHS England older people’s care | Shows value of integrated pathways, short-term support, urgent response, and system coordination. | Can become flow-driven if quality of life and carer reality are not measured. |
| Buurtzorg-inspired support | Shows value of relational continuity, small-team knowledge, and professional discretion. | Cannot be copied safely without training, governance, supervision, and funding fit. |
| Combined lesson | Older people need coordinated systems and known relationships. | One without the other leaves either fragmentation or unsupported discretion. |
NHS England’s older people’s care case shows the scale of the coordination problem. An older person’s journey may involve ambulance triage, emergency department assessment, frailty review, acute ward care, pharmacy, therapy, discharge planning, community nursing, adult social care, voluntary support, general practice, and family care. At each handoff, meaning can be lost. A note may say that the person is mobile with assistance, but the home may have stairs and no rails. A record may show that a carer is present, but the carer may be frightened of helping with transfers. A discharge summary may list medicines, while the person still does not know which tablets stopped.
Integrated care in action becomes valuable when it turns these fragments into one recovery path. The NHS England example of short-term intensive support for older people, including nursing, therapeutic assessment, and social care for up to ten days, illustrates a practical response to the gap between acute treatment and daily life. It recognizes that recovery is not a switch. It is a vulnerable period in which strength, confidence, nutrition, medication understanding, and household support all matter.
Frailty changes the meaning of time. A person who spends extra days in hospital may lose muscle strength, sleep poorly, become confused, or become less confident walking. A person discharged home without sufficient help may deteriorate just as quickly through falls, missed meals, medicine confusion, and fear. The NHS England direction toward frailty pathways and proactive care matters because frailty is not simply old age. It is a state of vulnerability in which small stressors can produce large decline. Management has to be earlier, more coordinated, and closer to the person’s ordinary life.
Urgent community response belongs in the case because many crises in later life develop at home before they become hospital admissions. A two-hour response model can make the difference between resolving a fall, infection concern, dehydration, or sudden functional decline at home and sending the person into hospital by default. The value is not only speed. It is the range of competence brought to the door: clinical assessment, therapy judgment, medication awareness, knowledge of social care, and a route for escalation when home is no longer safe.
Virtual wards for older people require the same caution. A virtual ward can provide hospital-level care at home when the person is suitable, the team can monitor and respond, and the household is not left carrying clinical work without preparation. The phrase ‘care at home’ can sound reassuring, but an older person’s home may lack broadband, heating, space, privacy, or a confident carer. In frailty care, suitability has to include cognition, sensory loss, falls risk, carer capacity, housing, and the ability to escalate. Digital monitoring cannot carry recovery alone.
Hospital discharge remains the sharpest test of NHS and social care coordination. CQC’s 2024/25 findings on delayed discharge causes show that community services, social care capacity, rehabilitation, reablement, and recovery services all affect whether a person can leave hospital safely. The public debate often asks why hospital beds are blocked. The better question asks why recovery capacity is not available when the person is ready to leave acute care. A bed is not released by paperwork. It is released by a safe plan that can actually happen.
Reablement deserves particular attention. It is not the same as task care. Task care may wash, dress, feed, and prompt. Reablement asks how the person can regain the ability to do more for themselves with graded support. The difference is ethical and economic. A person who regains enough confidence to walk to the bathroom, make tea, or manage simple personal care has recovered a portion of life. A system that lacks reablement may create dependence while believing it has delivered help.
Medicines safety is another NHS case issue. Older people often leave hospital with changed doses, new medicines, discontinued medicines, or advice that does not fit easily into the old routine. Polypharmacy can produce dizziness, confusion, dehydration, bleeding risk, constipation, falls, and readmission. The pharmacy link between hospital, GP, community pharmacy, carers, and home care staff has to be part of gerontological leadership. A discharge that is clinically complete but pharmacologically confusing remains unsafe.
The local authority interface is equally important. Adult social care assessment, care packages, housing adaptation, safeguarding, carers’ assessments, direct payments, provider capacity, and reablement commissioning all sit close to the older person’s actual life. Integrated care rhetoric has limited value if local authorities are brought into the conversation only when a discharge has already stalled. Joint planning requires shared visibility of care availability, equipment delay, carer risk, and neighbourhood support.
The voluntary and community sector also appears in the NHS England case as more than a decorative partner. Befriending, meals support, transport, falls-prevention classes, dementia groups, faith communities, and local charities can help prevent isolation and loss of confidence. These assets cannot replace statutory care when personal care, clinical assessment, or safeguarding is required. Yet they can make the difference between a person surviving at home and a person living with connection.
NHS England’s case evidence points to a practical leadership standard. Older people’s care works when hospital, community, social care, pharmacy, voluntary support, and family realities are governed together. It fails when each organization completes its own task while the person carries the gaps. The standard is not novelty. It is coordination that can be felt in the person’s day.
Chapter 5: Buurtzorg-Inspired Community Support and Relational Continuity
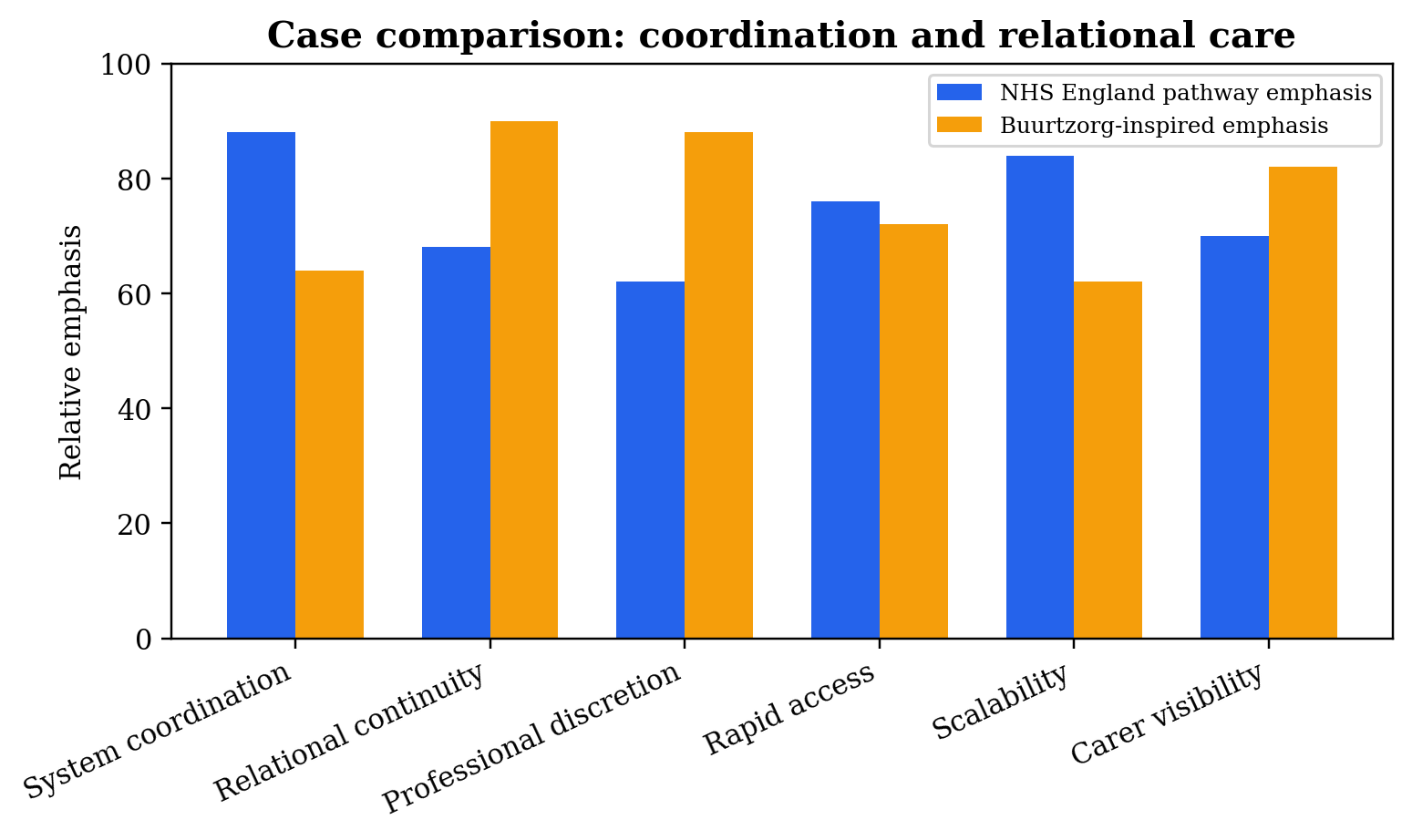
Figure 4. Case comparison: coordination and relational care. Copyright © June 2026 Juliet C. Nwaiwu / NYCAR. All rights reserved.
Buurtzorg-inspired home care is often admired because it offers a different image of care work: small teams, professional autonomy, fewer layers of bureaucracy, and relationships that are not constantly broken by staff rotation. The attraction is understandable. Much home care in strained systems becomes fragmented into visits measured by minutes, tasks, and contracts. Older people then experience care as a doorbell, a rushed worker, a completed task, and another unknown face next time. Relationship-centred practice asks for something more serious: knowing the person well enough to notice what is changing.
The evidence on Buurtzorg-derived models is careful rather than triumphant. Hegedüs and colleagues show that implementation outside the Netherlands involves adaptation, local constraints, and varied experience. De Bruin and colleagues similarly describe self-managing teams as promising but complex, with outcomes shaped by support, governance, training, and context. The point is not that Buurtzorg solves elderly care. The point is that it exposes a weakness in task-driven systems: care can be technically delivered while remaining relationally thin.
Continuity matters because older people often communicate distress indirectly. A person may say they are fine while eating less, moving more slowly, wearing the same clothes, or avoiding a room after a near fall. A familiar worker may know that this is not normal. A new worker may complete the scheduled task and leave. In dementia care, continuity can reduce anxiety and support recognition. In safeguarding, familiarity may allow disclosure. In medication support, a known worker may notice confusion before an error becomes harm.
Professional discretion is another lesson. Staff who know an older person well may need room to adjust the visit: spending extra minutes when confusion is higher, contacting a nurse when a wound looks wrong, asking about food when the fridge is empty, or noticing carer exhaustion. A system that allows only rigid task completion may look efficient while missing risk. Discretion, however, is not the same as unsupported improvisation. It requires training, documentation, supervision, escalation, and trust.
Small teams can support accountability because responsibility is local and visible. When a team knows its group of older people, the team can plan visits, share observations, and maintain relational memory. The model can reduce the sense that care is delivered by an anonymous workforce. Yet small teams can also become overloaded, isolated, or uneven if the wider system is weak. A self-managing team still requires data support, clinical links, safeguarding advice, workforce cover, and a route to specialist help.
Buurtzorg-inspired practice also changes the meaning of productivity. In a narrow time-and-task model, productivity may be measured by visits completed per hour. In relational care, productivity includes prevention: a fall avoided, an admission prevented, a carer kept from crisis, a medicine error caught, a lonely person reconnected. Those results are harder to count immediately, but they are not less valuable. Leadership has to protect measures that capture prevention rather than reward only visible activity.
Carers are central to this case. A relationship-based team is more likely to notice that the spouse is exhausted, that the daughter is missing work, or that family conflict is affecting care. Carer capacity cannot be assumed because a person is present in the house. Presence is not capacity. A spouse with arthritis may love the person deeply and still be unable to help safely at night. A son may visit daily and still not understand medicines. A care model that names carers as partners has to ask what they can realistically do.
Buurtzorg-inspired models also raise questions about equity. Relationship-based care may be easier to establish in areas with stable staffing, manageable travel times, good digital records, and local professional networks. Places with high deprivation, housing insecurity, rural distance, language barriers, and provider instability may find implementation harder. A serious leadership approach does not abandon the model in those places. It adapts the model while naming the additional investment required.
Technology has a specific place in this discussion. Digital care records, scheduling, remote monitoring, medication prompts, and risk flags can help small teams, especially when they reduce duplication and allow relevant information to travel. Technology becomes harmful when it pushes staff toward screens instead of observation, or when it turns care into data entry without judgment. A Buurtzorg-inspired approach does not reject technology. It asks whether technology protects the relationship or thins it out.
The case carries an important caution for England. Borrowed models can become slogans. A service can call itself person-centred while still rushing workers through short visits. It can announce self-management while leaving teams without the authority or support to act. It can praise continuity while commissioning care through contracts that break continuity every week. The lesson from Buurtzorg-inspired practice is not a brand name. It is the operational discipline of letting relationship, professional judgment, and local knowledge shape care.
When set beside NHS England’s integrated pathways, the Buurtzorg-inspired lens offers balance. System coordination without relationship can feel cold. Relationship without system coordination can become fragile. Older people need both: services that can coordinate risk across organizations, and workers who know enough about the person to see what the dashboard misses. Gerontological leadership is found in that combination.
Chapter 6: Quantitative Model and Scenario-Based Findings
Table 2. Scenario-based measures used in the study
| Measure | Formula | Interpretive use |
| Quality-of-life score | QoL = 0.25I + 0.20S + 0.20C + 0.20H + 0.15F | Profiles independence, safety, connection, confidence, and function. |
| Care-continuity index | CCI = known-team visits / total visits × 100 | Shows whether the person receives relationally consistent care. |
| Dependency ratio | DR = older population / working-age population × 100 | Supports local workforce and service planning. |
| Readmission-risk score | RRS = 0.30F + 0.25M + 0.20C + 0.15P + 0.10L | Identifies transitions requiring enhanced support. |
| Service-access time | SAT = average days from identified need to support start | Makes waiting visible as a care-quality risk. |
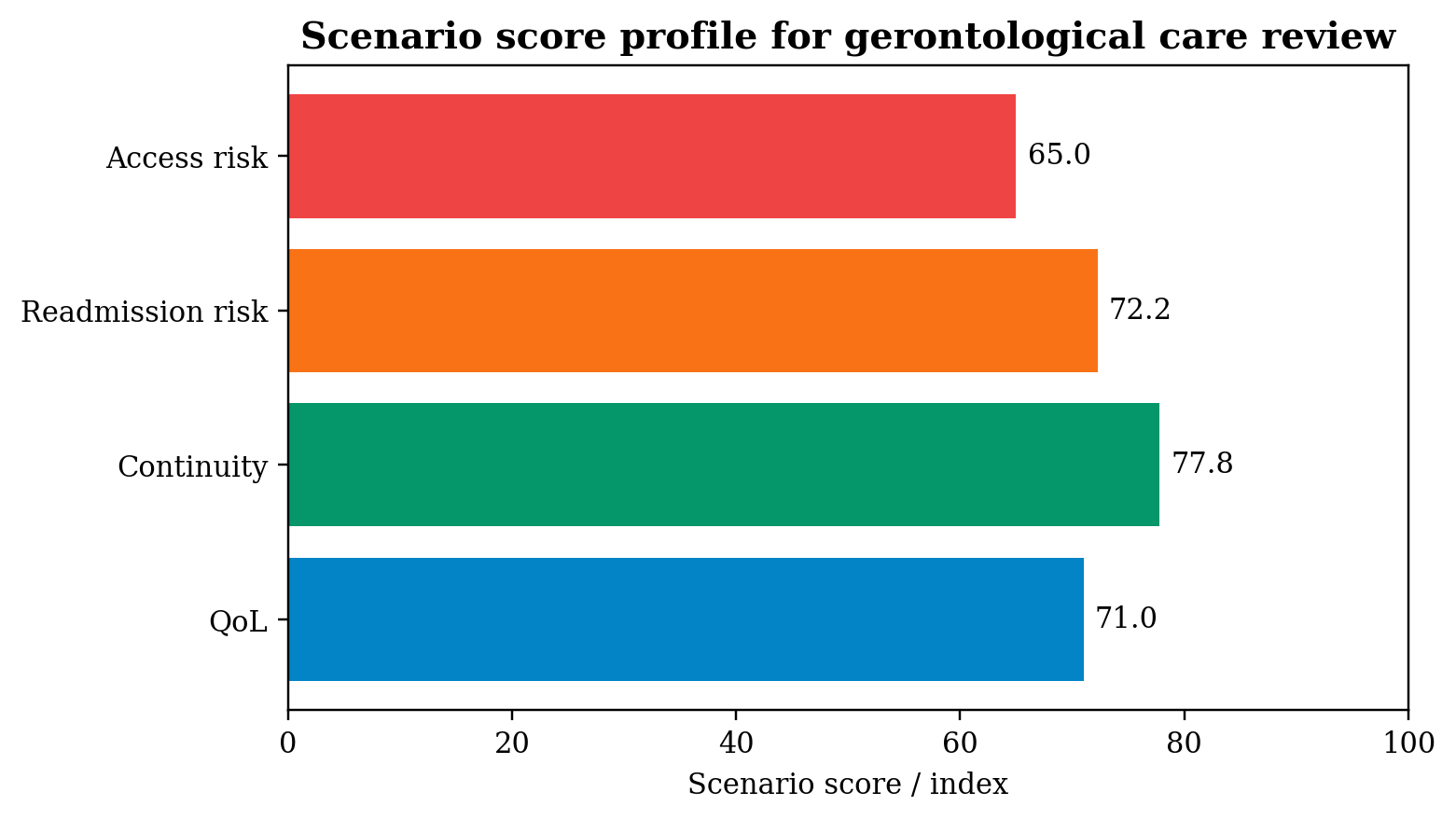
Figure 3. Scenario score profile for gerontological care review. Copyright © June 2026 Juliet C. Nwaiwu / NYCAR. All rights reserved.
Measurement in gerontological care requires humility. Numbers can reveal patterns, expose delay, and direct resources. They can also flatten a life if handled carelessly. The aim of this chapter is to use measurement as a way of asking better questions, not as a substitute for human judgment. The model developed here connects quality of life, continuity, access, readmission risk, demographic pressure, workforce stability, and carer evidence into a practical management frame.
Begin with the quality-of-life score. Suppose an older person has the following component scores after assessment: independence 72, safety 84, social connection 60, health confidence 70, and functional ability 68. Using QoL = 0.25I + 0.20S + 0.20C + 0.20H + 0.15F, the result is 0.25(72) + 0.20(84) + 0.20(60) + 0.20(70) + 0.15(68), which equals 71.0. The score is moderate, but the average is less important than the pattern. Safety appears relatively high; social connection is lower. A care review that notices only the total will miss loneliness.
That example shows why component-level interpretation matters. A person may be physically safe but emotionally isolated. Another person may be socially connected but at high falls risk. A person with dementia may have a supportive family but low confidence with unfamiliar workers. Managers need a dashboard that shows the profile, not only the number. Quality of life cannot be raised by one intervention if the limiting factor sits somewhere else.
The care-continuity index is also straightforward. If a person receives 18 visits in a month and 14 are delivered by known team members, CCI = 14 / 18 × 100, which equals 77.8 percent. Whether that is adequate depends on the person’s needs. It may be acceptable for a person requiring simple support and flexible coverage. It may be weak for a person with dementia, anxiety, or safeguarding risk. Continuity is not a sentimental preference. It has clinical and managerial meaning.
Readmission risk requires a wider view of transition. Consider frailty at 80, multimorbidity at 75, carer strain at 70, prior admission history at 60, and low service access at 65. Using RRS = 0.30F + 0.25M + 0.20C + 0.15P + 0.10L, the score is 72.25. A score at that level indicates a transition that requires active follow-up: medicines review, therapy, carer conversation, home safety check, nutrition, and escalation planning. The score does not predict one person’s future with certainty. It identifies a situation in which passive discharge would be reckless.
Service-access time turns waiting into evidence. If five older people wait 3, 5, 6, 8, and 13 days for home support, the average is seven days. The average hides the problem. A thirteen-day wait may be tolerable for a low-urgency social activity referral. It is dangerous after a fall, after discharge with mobility loss, or in a household where a frail spouse is managing alone. Access time has to be read beside risk. Delay is not a number in isolation. Delay is harm moving through time.
The dependency ratio offers a planning view. A locality with 28,000 residents aged 65 and over and 90,000 working-age residents has DR = 28,000 / 90,000 × 100, which equals 31.1 older residents per 100 working-age residents. This does not mean older people are a burden. It means local leaders need to plan for workforce, transport, housing adaptation, community assets, primary care, social care, and family support with population structure in mind. A place with a growing 85-plus population cannot plan services as if age distribution were unchanged.
The Integrated Gerontological Leadership Index brings these ideas together. Imagine a local system scoring quality-of-life review at 74, known-team continuity at 68, access timeliness at 62, readmission-prevention practice at 70, workforce stability at 58, and equity and carer evidence at 65. Using IGLI = 0.20Q + 0.20K + 0.15A + 0.15R + 0.15W + 0.15E, the score is 66.4. The number suggests a system with some working elements but visible weakness in access and workforce stability. The proper response is not a celebratory rating. It is a board-level question: what will change in the next quarter?
Model governance is as important as model design. Every component needs a clear definition. Independence cannot be scored differently by every assessor. Carer strain cannot be a tick box. Continuity cannot mean only that a provider organization is the same; it has to show whether the person sees known workers. Access time cannot be measured from referral acceptance if the person’s need was identified days earlier. Bad definitions produce neat numbers and poor care.
Equity testing is also required. A model may perform well for people who speak English, live with family, and have easy transport while undercounting risk among people living alone, renters, people with dementia, minority ethnic communities, rural residents, and people with sensory loss. Calibration by deprivation, ethnicity, language need, disability, rurality, living arrangement, and carer availability is not statistical decoration. It determines whether the model sees the people most likely to be missed.
The scenario findings support four management conclusions. Quality of life needs component analysis. Continuity requires actual measurement of known-team contact. Readmission risk has to include social and carer variables, not only diagnosis. Access delay has to be stratified by urgency. These conclusions may sound plain, but many systems still rely on narrow activity measures that hide exactly these issues.
The model also protects against a common managerial error: mistaking completed tasks for achieved care. A visit completed is not the same as a person washed with dignity. A discharge completed is not the same as recovery at home. A medication list sent is not the same as medication understood. A referral made is not the same as service received. The indicators in this chapter are useful because they push leaders closer to the lived consequences of their decisions.
Chapter 7: Leadership Practice, Carer Reality, and Dignity-Centred Implementation
The rebuilt Chapter 7 is not a quality-control note. It is the practical heart of the publication: how gerontological leadership can turn evidence, case learning, and measurement into better care. The chapter begins from a point that cannot be captured by policy language alone. Older people do not live inside service categories. They live inside homes, memories, bodies, routines, relationships, fears, and hopes. A leadership model that forgets that fact can be efficient and still inhumane.
Leadership in ageing care has to hold two forms of accountability at once. The service needs public accountability: budgets, waiting times, safeguarding, staffing, infection risk, hospital flow, and performance. The older person needs personal accountability: a worker who arrives, a plan that makes sense, a medicine that can be understood, a route for help, and a sense that the person’s preferences are not being treated as inconvenience. Good leadership refuses to trade one form of accountability against the other.
Carer reality is often where the system tells the truth about itself. Many care plans work only because a spouse, daughter, son, neighbour, or friend absorbs the gap. The document may call the person supported at home, while the real support is a tired family member checking tablets, washing clothes, cooking meals, changing sheets, helping with toileting, and sleeping lightly for fear of a fall. Unpaid care is not a footnote. It is a structural part of older people’s care, and it has to be assessed with honesty.
A carer assessment that asks only whether someone is available is not enough. Availability is not capacity. The right questions are more concrete. Can the carer lift or steady the person safely? Does the carer understand the medicines? Is the carer sleeping? Is paid work affected? Is there backup? Is the carer frightened? Has anyone explained what deterioration looks like? Is the carer consenting to the role or simply being assumed into it? These questions are not intrusive. They are safeguarding questions.
Dignity-centred implementation also requires attention to time. Older people’s services often harm by moving too slowly. Waiting for a commode, a rail, a medication review, a memory clinic, a falls assessment, or a care start can quietly narrow a life. The delay may appear as backlog in management reports; at home, it appears as urine on a chair because the toilet is unreachable, a skipped meal because standing is painful, or fear of bathing because no grab rail has arrived. Time is clinical, social, and moral.
Workforce leadership sits at the same level of importance. Relationship-based care cannot be built on constant staff turnover. Dementia care cannot thrive when workers change unpredictably. Reablement cannot succeed if therapy capacity is too thin. Home care cannot feel dignified when visits are impossibly short. Boards that discuss quality while ignoring workforce stability are discussing an abstraction. Quality arrives through people with skill, time, supervision, and fair treatment.
Professional discretion needs protection. Staff working with older people often see the real problem before the record does: a fridge with little food, bruising that does not match the explanation, a spouse close to collapse, a person who has stopped opening curtains, a house that has become too cold, a medicine bottle untouched. If the service allows only the planned task, that knowledge dies at the door. A mature service gives staff clear routes to raise concern and the authority to adjust care when risk changes.
Yet discretion without governance can also create danger. A worker improvising alone may miss safeguarding duties, clinical escalation, consent rules, or medication risk. The answer is not rigid bureaucracy. It is supported discretion: training, supervision, shared records, clear escalation, professional consultation, and review. Buurtzorg-inspired models are useful here because they value judgment, but the English context also requires careful alignment with regulation, commissioning, and safeguarding.
Housing has to enter implementation. Too many care plans assume the home is a neutral place. It is not. The home may contain stairs, loose rugs, poor lighting, cold rooms, narrow doors, inaccessible bathrooms, unsafe kitchens, mould, or overcrowding. A person may be discharged into a place that undermines the recovery plan from the first evening. Gerontological leadership has to connect health, social care, housing, occupational therapy, energy advice, and local government. Independence is not a personal trait alone; it is partly built by the environment.
Social connection belongs in the same conversation. Loneliness can reduce appetite, movement, motivation, sleep, and confidence. It can make a person less likely to report symptoms or attend appointments. A care system focused only on personal care visits may miss the fact that the person’s life has become smaller than the care plan admits. Faith groups, voluntary organizations, lunch clubs, libraries, befriending schemes, cultural associations, and neighbourhood networks are not clinical substitutes. They are part of the living ecology of ageing.
Digital tools require judgment. Remote monitoring, shared records, falls sensors, video consultations, medication prompts, and predictive risk systems can help. They can also exclude those with poor eyesight, dementia, hearing loss, arthritis, limited English, poverty, or low confidence with devices. Technology has to earn its place by making care safer, clearer, or more timely. It cannot be used to replace human presence where human presence is the intervention.
Implementation at board level needs a disciplined rhythm. A local ageing-care board can review a small number of signals each month: quality-of-life components, continuity, access delays by risk group, readmission-risk profiles, carer strain, workforce stability, reablement starts, dementia continuity, safeguarding themes, and patient/carer stories. A dashboard without stories can become cold. Stories without data can miss patterns. The board needs both.
Commissioning also has to change. Contracts that reward short visits and low price while ignoring continuity, travel time, carer support, and reablement outcomes cannot deliver relational care. Commissioners need evidence about what happens after the visit: whether function improves, whether the same workers are seen, whether carers remain stable, whether falls reduce, whether hospital returns are avoidable, and whether the person reports confidence. Cheap care that creates crisis elsewhere is not cheap.
Leadership development for gerontological care requires a different curriculum from generic management training. Leaders need to understand frailty, dementia, polypharmacy, safeguarding, falls, loneliness, housing, carer strain, workforce morale, and the politics of adult social care. They also need enough quantitative literacy to question dashboards and enough human literacy to hear what older people and carers are saying beneath polite answers. This is not a soft field. It is one of the hardest areas of public management because the consequences of weak leadership are intimate.
The chapter’s operating position is simple. Quality of life in later life improves when services are timely, relational, clinically aware, carer-conscious, and accountable. It declines when care becomes rushed, fragmented, defensive, or blind to the home. A gerontological leader is not judged by the elegance of a strategy. The leader is judged by whether the person at home experiences care as safe, known, and workable.
Chapter 8: Applied Care Scenarios: Dementia, Falls, Medicines, Housing, and Loneliness
Dementia care shows why gerontological leadership cannot rely on standard visit completion. A person living with dementia may not describe pain clearly, may resist help because the worker is unfamiliar, may lose confidence after a hospital stay, or may become distressed when routines change. A care plan that is clinically sensible on paper can fail if the person does not recognize the worker at the door or if instructions arrive in a form the person cannot retain. Dementia-sensitive leadership gives weight to routine, familiarity, calm communication, and the involvement of people who know the person’s ordinary behaviour.
Continuity is especially important in dementia because change may appear as a small deviation from baseline. A known worker may notice that a person who normally chats has become withdrawn, that food has gone uneaten, or that a room is being avoided. These observations can precede formal deterioration. In fragmented care, such signals may be missed until crisis occurs. The care-continuity index therefore has practical value; it gives leaders a way to protect familiar staffing for people whose safety depends on being known.
Falls are another test of leadership. A fall is rarely a random event in the life of a frail older person. It may reflect poor lighting, medication side effects, weak muscles, unsafe footwear, dehydration, urgency to reach the toilet, poor vision, clutter, or fear that has already changed walking patterns. A fall-prevention service that begins only after repeated incidents is late. Gerontological leadership treats falls as a system signal, bringing pharmacy, therapy, housing, vision, continence, nutrition, and carer advice into one plan.
The home environment turns falls prevention from a clinical topic into a practical one. A therapist may recommend exercises, but the person still has to cross a dark hallway at night. A medicine review may reduce dizziness, but the bathroom may remain unsafe. A falls pathway that cannot secure rails, lighting, footwear advice, and confidence-building support will be incomplete. This is where health care, social care, housing, and local government have to meet. The older person experiences their separation as risk.
Medication safety is equally central. Older people often live with polypharmacy, and hospital admission can change a familiar pattern. A medicine stopped on the ward may still be in the kitchen drawer. A new dose may be written correctly but misunderstood. A blister pack may not match the discharge summary. A carer may administer medicine without knowing why it changed. Medicines reconciliation is not a clerical task. It is one of the most practical safeguards in hospital-to-home care.
Pharmacists, GPs, community nurses, home care staff, hospital teams, older people, and carers all hold part of the medicine story. Leadership is needed because no one part sees the whole. A medication incident after discharge can be described as patient error, but often it reveals poor communication, unclear packaging, missing review, or a plan that assumed too much. The readmission-risk score needs a medication layer when local data allow it, especially for people with high-risk medicines, cognitive impairment, or recent dose changes.
Housing conditions may be the hidden determinant of independence. A person can be medically stable and still be unable to live safely where they are. Stairs may block access to the bedroom. A bathroom may require movements the person can no longer manage. Cold homes can worsen respiratory illness. Damp can affect health. Insecure tenancy can create anxiety and prevent adaptation. A housing-blind care plan is often a temporary illusion. It may keep the person home for a few days while the underlying hazard remains.
Older renters and people in poor housing deserve particular attention. Home ownership is often assumed in ageing policy, yet many older people live in rented, insecure, or unsuitable accommodation. Adaptation may be delayed by landlord consent, funding rules, or service fragmentation. A dignity-centred model treats housing adaptation, warmth, safety, and accessibility as part of care leadership, not as separate environmental background.
Loneliness can be harder to see than falls or medicines error, but its effect on daily life can be severe. An older person who sees no one may eat less, move less, speak less, and delay asking for help. Loneliness can also intensify anxiety after discharge. A person may technically receive care but still feel abandoned for most of the day. Social connection in the quality-of-life score is included because care cannot be reduced to bodily maintenance.
Community assets are valuable only when connected properly. A local church, mosque, lunch club, dementia café, walking group, volunteer driver scheme, or befriending project can help rebuild confidence. Yet referrals have to be realistic. Some older people need transport, reassurance, language support, or someone to go with them the first time. Handing someone a leaflet is not social prescribing. Leadership asks whether the connection happened.
Nutrition also belongs in applied gerontological care. Poor appetite, bereavement, dental problems, swallowing difficulty, poverty, and inability to shop can all weaken recovery. A fridge check may tell a story that a clinic note misses. Food is not only calories; it is routine, pleasure, culture, and independence. A care worker who has time to notice uneaten meals may prevent deterioration long before a hospital readmission occurs.
Safeguarding runs through all these scenarios. Dementia, frailty, dependency, poverty, and isolation can increase vulnerability to neglect, abuse, exploitation, and coercive control. Safeguarding is not a separate file opened only after a dramatic concern. It is a way of seeing risk in ordinary interactions. Known staff, careful records, respectful questioning, and clear escalation routes all matter. A service that rotates strangers through short visits may reduce its ability to hear what is really happening.
The scenarios show why the model in this paper remains deliberately broad. Quality of life cannot be separated from dementia care, falls prevention, medicines, housing, food, carers, and loneliness. Each issue can produce crisis on its own; together they shape whether later life feels manageable. Gerontological care leadership is the work of keeping those issues connected long enough for care to become real.
Chapter 9: Board Assurance, Commissioning, and Local Implementation
Table 4. Implementation assurance questions
| Area | Question for leaders | Evidence required |
| Discharge | Has the first week at home been made safe? | Care start, medicine plan, equipment, escalation route, carer contact. |
| Reablement | Is recovery support available early enough? | Start date, goals, therapist input, functional change. |
| Continuity | Do high-need older people see known workers? | Known-team visit rate and exceptions. |
| Carers | Is unpaid support sustainable? | Carer assessment, strain review, backup plan. |
| Equity | Who is being missed? | Outcomes by deprivation, rurality, ethnicity, language need, disability, and living arrangement. |
Figure 5. Implementation cycle for ageing-care leadership. Copyright © June 2026 Juliet C. Nwaiwu / NYCAR. All rights reserved.
A local board responsible for older people’s care needs a different kind of assurance from the one used for simple activity reporting. It needs to know whether the system is protecting people during the points where harm usually enters: discharge, first days at home, medication change, care-start delay, carer overload, falls risk, dementia-related distress, and delayed reablement. A board pack that reports only contacts, visits, and waiting lists will not show whether older people are living safely.
Board assurance begins with a small number of disciplined questions. Are frail older people receiving timely assessment? Are high-risk discharges followed up within the agreed window? Are medication changes reviewed? Are carers being assessed where care plans depend on them? Are people with dementia receiving continuity? Are reablement starts delayed? Are access delays worse in rural areas or deprived neighbourhoods? Are readmissions linked to known service gaps? These questions turn leadership from presentation into accountability.
Commissioning has to carry the same seriousness. Contracts shape care. A contract that pays for short task visits will produce short task visits. A contract that ignores travel time will punish continuity in spread-out areas. A contract that tracks only visit completion will not capture whether the person regained confidence. Commissioners need to build continuity, reablement outcomes, carer involvement, safeguarding responsiveness, and equity into the way services are purchased and reviewed.
Provider stability is also a commissioning issue. Older people suffer when care markets are fragile. A provider collapse, sudden staffing loss, or rota failure can throw a household into immediate risk. Local authorities and integrated care systems need early warning about provider stress, workforce turnover, quality deterioration, and financial fragility. Market oversight may sound distant, but older people experience it when a familiar worker disappears or a care package cannot start.
Data sharing requires careful governance. Health and social care teams need enough information to coordinate care, but older people retain rights over privacy and dignity. Shared records can reduce repeated questioning, missed medication details, and duplicated assessments. They can also expose sensitive information if poorly controlled. A lawful, proportionate data-sharing model is part of gerontological leadership because safe care often depends on information travelling with the person.
Local implementation can begin with one pathway rather than an entire system redesign. A place may select older adults discharged after a fall, people living with moderate or severe frailty, or people referred to urgent community response. The local team can define variables, collect data, test the quality-of-life profile, measure continuity, review carer strain, and track access time. Starting small allows leaders to see where the record fails before scaling the model.
Patient and carer involvement has to be built into implementation from the beginning. A metric designed without older people may miss what they value. Some may prioritize staying home; others may prioritize pain control, bathing safely, seeing family, or not being a burden. Carers may identify gaps that staff cannot see, such as night-time fear, confusion around medicines, or the emotional cost of repeated calls. Co-design is not ceremony. It is a way of finding the real problem.
Workforce involvement is equally important. Frontline staff know where the pathway breaks. They know when travel time is unrealistic, when documentation duplicates, when equipment delays are routine, when hospital discharge information is poor, and when care packages assume impossible work. A leadership model that ignores staff knowledge will design neat processes that fail at the doorstep. Staff need not only instructions but a voice in improving the system.
Financial stewardship also belongs in the model. Dignity-centred care costs money, but poor care carries its own costs: hospital readmission, longer-term dependency, carer breakdown, safeguarding investigation, emergency placement, ambulance use, and loss of trust. Reablement, continuity, and early support may look expensive when viewed in one budget line and economical when viewed across the whole pathway. Integrated care finance has to follow the person rather than defend organizational silos.
Equity assurance requires disaggregated data. Older people in deprived neighbourhoods may face worse housing, fewer informal resources, lower digital access, and more difficulty securing transport. Minority ethnic older people may face language barriers, culturally inappropriate care, or lower trust in services. Rural older people may face distance, thin provider markets, and poor public transport. A single average can hide all of this. Board assurance needs to ask where the model works least well.
Digital transformation requires a similar equity test. A remote monitoring service that assumes a smartphone, broadband, English literacy, good vision, and family support will miss many older people. Digital records may help professionals, but digital self-management may fail for those with cognitive impairment or poverty. Technology can support ageing care when it reduces delay, improves information flow, and protects safety. It becomes unjust when it shifts work onto people least able to carry it.
Implementation also needs a learning rhythm. Every month, the team can review cases where the pathway worked and cases where it failed. The review can ask what was known, who knew it, what action followed, and what blocked improvement. A fall after discharge, a carer crisis, or a medication incident is not only an event. It is evidence. The best local systems turn such evidence into changed practice.
External accountability can reinforce local learning. CQC inspection, public reporting, health scrutiny committees, patient participation groups, and voluntary organizations all create pressure to make care visible. Yet accountability becomes useful only when it looks beyond headline activity. Regulators and local leaders need to ask about continuity, dignity, reablement, carer strain, and lived outcomes. Older people’s care cannot be assessed properly by counting the wrong things accurately.
Board assurance is finally a moral practice. A board that has seen evidence of delayed care, carer strain, poor continuity, or avoidable readmission cannot treat those findings as neutral data. Each point represents someone’s mother, father, neighbour, friend, or future self. The work of leadership is to connect numbers with responsibility before the next crisis makes the connection unavoidable.
Chapter 10: Recommendations and Final Position
The recommendations in this publication follow from the evidence rather than from aspiration. Local systems can begin by making quality of life a formal outcome in older people’s care. This means recording more than activity. Independence, safety, social connection, health confidence, and functional ability need a place in review conversations. A measure does not need to be complicated to be useful. It needs to be understood, repeated, and acted on.
Integrated care systems can create a gerontological care dashboard that combines quality-of-life profiles, care continuity, access time, readmission risk, reablement starts, carer strain, and workforce stability. The dashboard has value only when it changes decisions. If the data show poor continuity for people living with dementia, commissioning and rota design have to respond. If access delays cluster in one locality, the board has to ask why. If carer strain predicts readmission, the response cannot be another leaflet.
Every older person discharged from hospital with functional, cognitive, medication, or social risk requires a named transition owner. Responsibility cannot dissolve across teams. The transition owner does not personally deliver every service; the role is to ensure that medicine changes, equipment, care start, reablement, carer contact, and escalation routes are confirmed. Discharge becomes safer when the system knows who is watching the first days at home.
Reablement and rehabilitation need protection as recovery infrastructure. They are often treated as optional when budgets tighten, yet they can decide whether a person regains independence or enters long-term dependence. Local systems can track days from discharge to reablement start, proportion of eligible older people receiving reablement, functional gains, carer impact, and readmission patterns. The value of reablement is not only bed flow. It is restored life.
Continuity deserves explicit commissioning. Home care contracts can include known-team targets for older people with dementia, high anxiety, safeguarding concern, or complex medication. Scheduling systems can protect relational continuity rather than disrupt it for administrative convenience. Provider performance can include continuity data alongside punctuality and visit completion. A familiar face is not a luxury in gerontological care.
Carer support has to move from informal gratitude to formal governance. Carer capacity, confidence, health, sleep, work pressure, and backup need review where a care plan depends on unpaid labour. Local systems can track carer assessments, emergency respite access, training offered, and carer-reported strain. The ethical point is direct: a service that depends on carers owes them evidence-based support.
Housing and adaptation pathways need tighter connection with health and care. Falls prevention, rails, lighting, heating, accessible bathrooms, clutter reduction, and equipment delivery can determine whether the person stays safe. Delays in housing adaptation belong on the same risk map as care delays. Occupational therapy and housing officers need earlier involvement where the home environment is part of the risk.
Virtual wards and remote monitoring for older people need suitability rules that include cognition, sensory function, home safety, carer capacity, digital access, and face-to-face response availability. A remote model that works for one household may be unsafe for another. Local evaluation needs to include escalation calls, failed readings, transfer back to hospital, patient confidence, carer strain, and equity by deprivation, language need, rurality, and disability.
Workforce stability is not an administrative concern. It is a care-quality determinant. Local systems can monitor vacancy rates, turnover, agency use, sickness, training, supervision, travel time, and visit length. Relationship-based care will remain language if workers are constantly leaving or if visits are too compressed for dignity. Investment in workforce is investment in quality of life.
Professional training needs to be grounded in real ageing-care situations. Staff need scenarios on delirium, dementia distress, hidden carer strain, medicines confusion, falls fear, malnutrition, safeguarding, loneliness, and culturally sensitive support. Training becomes useful when it helps staff recognize risk earlier and communicate with older people and carers without patronizing them.
Post-incident learning can be adapted from patient-safety practice. When an older person is readmitted, falls after discharge, experiences a medicine incident, or reaches carer crisis, the review can ask what warning signs existed. Did the care plan assume too much? Was the first visit late? Were medicines understood? Was continuity weak? Was housing risk known? The goal is not blame. The goal is to identify the place where the system could have acted sooner.
Research can develop this publication further through local empirical evaluation. Future studies could estimate the relationship between continuity and readmission, reablement timing and functional recovery, carer strain and emergency calls, or housing adaptation delay and falls. Mixed-methods research with older people and carers would add depth to the scenario model. The present paper gives a framework; local evaluation would test and refine it.
The final position is that gerontological care leadership requires more than compassion. Compassion without organization becomes fragile. Organization without compassion becomes cold. Older people need systems that are both humane and capable: services that arrive on time, know the person, understand risk, include carers, protect dignity, and learn from failure. Ageing care is one of the clearest tests of whether public service can remain personal at scale.
A society that lives longer has not solved ageing; it has created a responsibility. The responsibility is to make later life livable where possible, protected where necessary, and respected always. Juliet C. Nwaiwu’s study contributes to that responsibility by giving managers a practical language for connecting quality of life, continuity, access, and leadership. The measure of success is not whether the system sounds integrated. The measure is whether older people feel the difference in ordinary life.
One more point belongs in the final position: older people’s care requires memory. Services often reorganize, rename pathways, replace teams, and redraw accountability maps. The older person and carer may then meet the same problem under a new label. Institutional memory protects against that churn. Local systems can preserve what was learned from serious incidents, delayed discharges, failed care starts, provider collapse, missed dementia distress, and carer crisis. A service that cannot remember its own failures will repeat them politely.
Research and practice also need better language. Terms such as independence, choice, care at home, and integrated care sound positive, but each can hide pressure. Independence can become abandonment when support is absent. Choice can become a burden when only poor options are available. Care at home can become unpaid family labour when the formal service is thin. Integrated care can become a meeting structure that never reaches the person. Gerontological leadership has to test its words against lived experience.
Ageing care also has an intergenerational meaning. Younger people are not outside the issue; they are future older people, current carers, workers in the care economy, taxpayers, daughters, sons, neighbours, and colleagues. A society that underfunds, undervalues, or fragments older people’s care is not saving itself from cost. It is transferring cost into hospitals, families, low-paid work, and private distress. Sound leadership brings those hidden costs back into view.
Juliet C. Nwaiwu’s publication is positioned as a master’s-level contribution because it offers an applied, evidence-grounded framework rather than an abstract theory of ageing. Its value lies in the practical combination of NHS England pathways, Buurtzorg-inspired relational care, quality-of-life measurement, continuity tracking, carer recognition, and board-level accountability. The framework can be adapted by local systems, care providers, graduate researchers, and policy-facing managers who want ageing care to be measurable without becoming mechanical.
The lasting claim is deliberately plain. Older people do not ask systems to be perfect. They ask, often quietly, that help arrives when promised, that workers listen, that medicines make sense, that carers are not left alone, that home is made safer, that recovery is possible, and that frailty does not erase personhood. A care system that meets those tests has done something more difficult than producing a strategy. It has made public responsibility visible in private life.
The model also gives NYCAR a defensible publication standard for applied care leadership: the mathematics is transparent, the evidence boundary is visible, and the argument remains close to the person whose life is affected by each decision. That combination is what separates a useful master’s research publication from a broad essay on ageing.
Used carefully, the framework can help local leaders resist two failures at once: the sentimental failure that speaks warmly about older people without changing services, and the technical failure that measures services while forgetting the person. NYCAR’s standard sits between those errors. It expects evidence, but it also expects evidence to serve dignity.
Appendix A: Measurement Assurance and Local Data Rules
Local use of the model requires rules that are more precise than the language of the publication. A quality-of-life score is only useful when assessors understand the components in the same way. Independence, for example, cannot be reduced to whether the person can perform one activity. It may include washing, dressing, toileting, cooking, moving around the home, leaving the house, managing small decisions, and expressing preferences. Local systems can define independence through a short set of observable domains and then allow the older person to identify which domain matters most to them.
Safety also requires definition. A safe home is not only a home without obvious hazards. Safety includes falls risk, medication clarity, nutrition, heating, infection risk, safeguarding, cognitive safety, equipment availability, and whether help can be summoned in time. A person may be safe at noon when a worker is present and unsafe at night when the toilet is far away and pain is worse. Local assessment needs to consider the full day, not only the professional visit.
Social connection is often under-measured because it looks less urgent than medication or mobility. Yet social disconnection can affect nutrition, mood, motivation, adherence, and help-seeking. A local tool can ask whether the person has meaningful contact, whether that contact is wanted, whether transport or fear prevents participation, and whether bereavement has changed the person’s routine. Counting contacts alone may be misleading; a person can have many brief professional visits and still be deeply lonely.
Health confidence needs careful wording. It does not mean the person understands every medical detail. It means the person has enough practical understanding to know what is happening, what to do next, whom to contact, and what signs require help. A person leaving hospital with new medicines and a complicated follow-up plan may have low health confidence even when the plan is clinically correct. Plain-language communication becomes part of the intervention.
Functional ability can be assessed through mobility, transfers, personal care, continence, meal preparation, and ability to participate in ordinary routines. Functional ability is not static. It may improve with reablement or decline quickly after bed rest, infection, pain, or fear of falling. Local data systems can record change rather than only a single score. A score that moves from 48 to 60 may represent a real gain in the person’s life, even when the person remains far from full independence.
Carer strain requires its own measurement. Local systems can use a short scale that records sleep disruption, physical tasks, emotional stress, work impact, confidence, availability of backup, and willingness to continue. The measurement needs to be repeated because carer strain changes. A spouse may cope during the first week after discharge and become exhausted in the third. A daughter may appear available until employment pressure makes the role unsustainable. Static carer data can create false assurance.
Known-team continuity also needs local rules. A visit by the same provider is not always a known-team visit. The older person may see different workers employed by the same agency. For this model, a known-team visit means the worker is known to the person or belongs to a small team familiar with the person’s care plan, risks, preferences, and communication needs. The definition has to be practical enough for providers to record and meaningful enough for older people to recognize.
Access time is measured from the point at which need is identified, not from the point at which a service accepts referral. If an older person waits three days before referral and five days after referral, the lived access time is eight days. Systems often measure the part of the delay they own. The person experiences the whole delay. Measurement has to follow the person rather than protect organizations from uncomfortable data.
Readmission-risk scoring needs clinical oversight. Frailty scores, multimorbidity, carer strain, prior admissions, and service access all contribute to risk, but the model can be strengthened with local variables such as medication burden, delirium history, falls, continence, nutrition, housing risk, cognitive impairment, and palliative status. The model cannot be expanded endlessly. Too many variables can make it harder to use. Local teams need a compact score that still sees the major hazards.
Data quality can be checked through audit. A monthly sample of records can test whether frailty was scored consistently, whether carer strain was documented where relevant, whether access time was measured from the correct point, and whether known-team continuity was recorded accurately. Audit cannot become punitive paperwork. It reveals whether the system knows enough to govern care.
Missing data function as information. If no carer assessment appears for a person whose plan depends on family support, the absence is not neutral. If housing risk is blank, leaders cannot assume the home is safe. If social connection is unrecorded, loneliness has not disappeared. A useful dashboard can include a missing-data rate because what the system fails to record may expose what it fails to value.
Local implementation also requires consent and privacy safeguards. Older people need to understand how information about their care, home, risks, and family support will be used. Some data are sensitive: dementia diagnosis, safeguarding concerns, family conflict, financial hardship, housing condition, and carer capacity. Data sharing has to be lawful, proportionate, secure, and explained. Better coordination cannot be purchased by careless privacy practice.
The model belongs in review with older people and carers before live use. They can identify words that feel patronizing, questions that miss the point, and scores that fail to capture what matters. A person may say that the measure asks about walking but not about fear of leaving the house. A carer may say that the form asks about tasks but not about emotional strain. These comments improve the model because they return it to lived reality.
Staff training is part of measurement assurance. A worker asked to score social connection or carer strain needs more than a form. They need examples, prompts, supervision, and a safe way to discuss uncertainty. Training can use realistic scenarios: a person who says they are fine but has lost weight, a carer who jokes about exhaustion, a person with dementia who refuses a new worker, or a home that is tidy but unsafe at night. The goal is thoughtful consistency, not mechanical scoring.
Thresholds are set locally and revised after evidence accumulates. A readmission-risk score above a given level might trigger a follow-up call within twenty-four hours, pharmacist review, reablement discussion, or carer contact. A low continuity score for a person with dementia might trigger rota review. A high access delay for urgent support might trigger escalation to the integrated care board. The threshold matters only if action follows.
Outcome review compares prediction with reality. If a person scored low risk and was readmitted, the case can be reviewed to identify what the model missed. If a person scored high risk and recovered well, the review can ask which support worked. This learning loop prevents the model from becoming fixed doctrine. Good local governance treats every mismatch as an opportunity to improve judgment.
The appendix also clarifies the publication’s mathematical restraint. The formulas are simple because the purpose is practical use in health and social care management. A more complex model may be suitable for statistical research, but a local service needs indicators that frontline staff, managers, board members, older people, and carers can understand. Clarity is an ethical requirement when measures influence care.
No score in this model has authority over dignity. A person’s stated priorities, cultural values, family context, and right to refuse support remain central. Measurement helps the system see risk and plan care. It does not erase autonomy. The best use of data in gerontological leadership is to make support more timely, more personal, and more accountable.
References
Age UK. (2024). The state of health and care of older people in England 2024. Age UK.
Age UK. (2025). The state of health and care of older people in England 2025. Age UK.
Allan, S., Roland, D., Malisauskaite, G., Jones, K., Forder, J., & Wittenberg, R. (2021). The influence of home care supply on delayed discharges from hospital in England. BMC Health Services Research, 21, Article 1297. https://doi.org/10.1186/s12913-021-07341-7
Care Quality Commission. (2025). The state of health care and adult social care in England 2024/25. Care Quality Commission.
Centre for Ageing Better. (2025). The state of ageing 2025. Centre for Ageing Better.
Dambha-Miller, H., Simpson, G., Hobson, L., Chapman, J. L., & Damery, S. (2021). Integrated primary care and social services for older adults with multimorbidity in England: A scoping review. BMC Geriatrics, 21, Article 674. https://doi.org/10.1186/s12877-021-02618-8
de Bruin, J. H., Doodkorte, R. J. P., Sinervo, T., & Clemens, T. (2022). The implementation and outcomes of self-managing teams in elderly care: A scoping review. Journal of Nursing Management, 30(8), 4549–4559. https://doi.org/10.1111/jonm.13836
Department of Health and Social Care. (2025). Adult social care in England, monthly statistics: January 2025. Department of Health and Social Care.
Hegedüs, A., Schürch, A., & Bischofberger, I. (2022). Implementing Buurtzorg-derived models in the home care setting: A scoping review. International Journal of Nursing Studies Advances, 4, Article 100061. https://doi.org/10.1016/j.ijnsa.2022.100061
National Institute for Health and Care Excellence. (2023). Integrated health and social care for people experiencing homelessness. NICE.
NHS England. (2023). Proactive care: Providing care and support for people living at home with moderate or severe frailty. NHS England.
NHS England. (2024). Integrated care in action: Older people’s care. NHS England.
NHS England. (2025). Best practice guide for NHS frailty pathways. NHS England.
NHS England. (2025). Urgent and emergency care plan 2025/26. NHS England.
Norman, G., Bennett, P., Vardy, E. R. L. C., Clarke, A., & others. (2023). Virtual wards: A rapid evidence synthesis and implications for the care of older people. Age and Ageing, 52(1), afac319. https://doi.org/10.1093/ageing/afac319
Office for National Statistics. (2023). Profile of the older population living in England and Wales in 2021 and changes since 2011. Office for National Statistics.
Office for National Statistics. (2025). Estimates of the very old, including centenarians, UK: 2002 to 2024. Office for National Statistics.
Skills for Care. (2025). The state of the adult social care sector and workforce in England. Skills for Care.
World Health Organization. (2015). World report on ageing and health. World Health Organization.
World Health Organization. (2021). Decade of healthy ageing: Baseline report. World Health Organization.
World Health Organization. (2024). Integrated care for older people: Guidance and implementation resources. World Health Organization.