Foresight, Results Discipline, and Resilience in Multilateral Operations
Research Publication by Blessing Chima-Chiemezie
New York Center for Advanced Research (NYCAR)
Institutional Review
June 2026
Publication Number: NYCAR-TTR-2026-RP051
DOI: https://doi.org/10.5281/zenodo.20582883
Peer Review Status:
This research paper has been reviewed under the internal editorial framework of the New York Center for Advanced Research (NYCAR) and The Thinkers’ Review. The review assessed doctoral-level coherence, source integrity, strategic-risk relevance, UN-facing policy value, regulatory precision, quantitative-model suitability, APA 7th alignment, and institutional relevance.
Abstract
Strategic risk management has become a central test of multilateral leadership because contemporary crises no longer arrive in sequence. Conflict, climate shock, food insecurity, forced displacement, debt distress, public health threats, cyber exposure, disinformation, and political fragmentation increasingly reinforce one another. In that environment, the United Nations system does not suffer from a shortage of strategies. It suffers, as many large public systems do, from the harder problem of execution under uncertainty: how to convert risk signals, foresight, evidence, partner knowledge, and ethical safeguards into timely choices before delay damages results.
This doctoral research examines strategic risk management as a leadership discipline for United Nations system performance and for organizations seeking credible alignment with UN priorities. It argues that risk cannot remain a compliance register owned by auditors, nor can foresight remain a reflective exercise detached from budget authority. Risk leadership belongs inside mandate interpretation, programme design, procurement, finance, safeguarding, digital governance, evaluation, public communication, and country-level decision-making. It draws on official and public materials from UN 2.0, the Pact for the Future, the Joint Inspection Unit’s enterprise risk management review, UNDP risk-informed development practice, WFP strategic and innovation materials, UNHCR results and evaluation materials, UNICEF strategic planning, WHO health emergency preparedness materials, and United Nations system management and resilience work. These sources are treated as management evidence with different evidentiary weights: policy statements show institutional intent, strategic plans show planned direction, management and results frameworks show implementation logic, and evaluations or oversight reports offer stronger evidence of organizational friction.
The research develops four applied diagnostic tools. The Strategic Risk Leadership Index tests whether mandate clarity, risk sensing, foresight use, decision rights, resource mobility, partner coordination, evidence learning, safeguards, stakeholder trust, and decision lag are aligned. The Risk-Adjusted Results Delivery model tests whether reported outputs remain credible after quality, equity, sustainability, residual risk, and potential harm are considered. The Decision-Lag Diagnostic examines the time lost between signal recognition and field response. The Partner Trust and Accountability Score treats partnership quality as a risk control rather than a diplomatic slogan. The research paper then applies these tools to case readings of WFP, UNHCR, UNDP, UNICEF, WHO, and system-wide reform agendas. Its core conclusion is direct: the United Nations system will not be judged by how often it names volatility, but by whether it can turn risk intelligence into decisions that protect people, preserve mandate integrity, explain trade-offs, and learn fast enough to matter.
Keywords: strategic risk management; United Nations; UN 2.0; foresight; enterprise risk management; risk-informed development; results-based management; humanitarian operations; resilience; data governance; accountability; NYCAR.
Contents
List of Tables
Table 1. Strategic risk domains and leadership control questions 24
Table 2. Strategic Risk Leadership Index components 29
Table 3. Case-study matrix 44
Table 4. Decision-lag stages and corrective actions 56
Table 5. Recommendations and evidence for oversight 79
List of Figures
Figure 1. Strategic Risk Leadership Index: component weights. 31
Figure 2. Partner Trust and Accountability Score: component weights. 35
Figure 3. Decision-Lag Diagnostic: illustrative elapsed time across the seven stages. 33
Chapter 1: Introduction: From Risk Awareness to Decision Accountability
Strategic management inside the United Nations system cannot be reduced to corporate planning with diplomatic vocabulary attached. The operating field is too exposed and too politically mediated. A UN country team may work where drought has already weakened livelihoods, conflict has broken public administration, debt pressure has narrowed fiscal space, misinformation has damaged trust, and humanitarian access depends on negotiations that can change overnight. A headquarters strategy can describe these pressures, but the field question is sharper: when the assumptions fail, who is authorized to change the plan?
The argument begins with a practical diagnosis. The United Nations system has no shortage of strategies, compacts, plans, frameworks, guidance notes, results matrices, risk registers, and reform agendas. The problem is not the absence of institutional language. The problem is the distance between language and action. A risk register can exist without moving money. A foresight paper can be admired without changing procurement timing. A results framework can report outputs while field staff still carry unresolved delivery risks. That distance – between awareness and decision – is where strategic risk management becomes a leadership problem.
Risk management is often placed in a procedural corner. It is associated with compliance, audit, internal control, fraud prevention, insurance, and reputational exposure. Those functions are essential, but they do not exhaust the meaning of risk in multilateral work. For the UN, risk is also about protection failure, exclusion, loss of humanitarian access, unsafe digital practice, weak partner support, field staff exposure, poor targeting, slow escalation, and the erosion of public trust. Risk is therefore not only something to be avoided. It is information about what can prevent a mandate from being delivered.
The central claim of this research is that strategic risk management should be treated as decision accountability under uncertainty. This definition is deliberate. “Strategic” means the risk concerns mandate delivery, legitimacy, institutional capacity, or the protection of people affected by action or inaction. “Management” means the organization has a route from signal to decision, from decision to resource movement, and from action to learning. “Accountability” means leaders can explain what they knew, when they knew it, what authority they used, what trade-offs they accepted, and what safeguards protected affected populations.
UN 2.0 gives this question current force. The Secretary-General’s UN 2.0 agenda emphasizes stronger capabilities in data, digital solutions, innovation, foresight, and behavioural science, underpinned by a forward-looking culture (United Nations, 2023). These capabilities are not ornamental. Data without judgment can mislead. Digital transformation without inclusion and cybersecurity can create new vulnerabilities. Innovation without adoption becomes a pilot culture. Foresight without budget authority becomes a seminar. Behavioural insight without ethics can cross into manipulation. The promise of UN 2.0 is real, but only if these capabilities enter the decision system.
The Pact for the Future broadens the same challenge. Adopted at the Summit of the Future in September 2024, it brings together sustainable development, peace and security, science and technology, digital cooperation, youth and future generations, and global governance reform (United Nations, 2024). The Pact is relevant to risk management because it converts the future from a rhetorical horizon into a governance responsibility. An institution that claims duties to future generations must ask whether current funding cycles, procurement rules, partner agreements, data practices, and programme incentives are building resilience or consuming it.
The research is UN-facing but not ceremonial. It assumes that the UN system contains serious professionals working under severe constraints. It also assumes that good intentions do not remove the need for sharper management discipline. Multilateral organizations are morally burdened because their mandates concern human lives, rights, peace, development, and global cooperation. They are administratively burdened because they must act through member-state politics, earmarked funding, procurement rules, security protocols, implementing partners, inter-agency coordination, and public scrutiny. Strategic risk management lives inside that mixture.
For NYCAR purposes, the research aims to serve three audiences. The first is the academic reader interested in risk governance, public administration, humanitarian operations, and institutional performance. The second is the UN-facing practitioner who needs usable tools rather than theory alone. The third is the institutional partner seeking credibility with UN priorities and therefore needing to demonstrate not only ambition, but safeguards, evidence discipline, financial control, partner responsibility, and learning capacity.
1.1 Background and Research Problem
The contemporary operating environment is best understood as compound risk. Food insecurity is not only a food problem when conflict disrupts supply routes, climate shock damages production, inflation raises prices, debt pressure reduces public spending, and misinformation undermines public confidence in assistance. Forced displacement is not only a protection problem when host communities face housing pressure, public services are overstretched, borders become politically contested, and digital registration systems raise privacy risks. Health emergencies are not only epidemiological problems when rumours spread faster than guidance, health workers are attacked, and fragile systems lose staff and supplies.
The United Nations was created for problems that exceed the capacity of any one state. Yet the present period stresses the management side of multilateralism in an unusual way. Crises overlap, political consensus is harder to maintain, funding is unstable, public trust is contested, and digital tools change both the possibilities and the risks of intervention. Mandate authority remains necessary, but it is no longer sufficient. The question is whether institutions can act with enough speed, discipline, and ethical clarity when the operating picture changes faster than formal planning cycles.
The research problem is the gap between strategic risk language and risk-informed execution. Many organizations can name risks. Fewer can demonstrate that risk analysis changes priorities, deadlines, staffing, security posture, partner oversight, budget allocation, procurement, data governance, or public communication. This problem is intensified in the UN system because authority is distributed. Headquarters, regional bureaus, country offices, donors, governing bodies, host governments, implementing partners, and affected communities all shape outcomes, but they do not sit in one clean chain of command.
Decision lag is the practical symptom of this gap. Risk signals often appear before action. Field teams may notice that access is deteriorating. Local partners may warn that community trust is weakening. Procurement officers may detect supply fragility. Protection teams may identify patterns before formal complaints increase. Data officers may see a cyber or privacy risk before programme managers understand its operational consequences. Delay can come from unclear escalation, donor restrictions, legal caution, procurement rules, insufficient flexible funding, or fear that bad news will be punished. Whatever the cause, delay has consequences. In high-risk settings, a late decision can look very much like a wrong decision.
A second symptom is results distortion. Results-based management is indispensable for accountability, but output reporting can flatter performance if it is detached from risk. A programme can meet numerical targets while failing marginalized groups. A digital tool can accelerate registration while excluding people without documents or connectivity. A resilience project can deliver training while local systems remain unable to absorb the next shock. Strategic risk management asks whether the result is not only delivered, but dependable, equitable, safe, and sustainable under stress.
A third symptom is hidden risk transfer. Localization, partnership, efficiency, and digital modernization can all be positive. They can also move risk downward if they are pursued without safeguards. A local partner may be asked to deliver in an insecure area without adequate overhead, insurance, duty-of-care support, data systems, or cash-flow reliability. A shared digital platform may reduce duplication while concentrating cybersecurity exposure. A cost-saving measure may reduce redundancy that later proves essential in crisis. This research treats those trade-offs as central rather than secondary.
1.2 Aim, Objectives, and Research Questions
The aim of the research is to develop a doctoral-level strategic risk management framework for United Nations system performance and for organizations that seek to work credibly with UN priorities. The research does not audit a single UN entity. It does not claim internal access. It uses public materials to construct a rigorous applied framework that can help leaders examine whether risk intelligence is changing decisions.
The study pursues five objectives. It defines strategic risk management as a leadership capability rather than a compliance file, then reads UN 2.0, the Pact for the Future, enterprise risk management sources, results-based management materials, evaluation evidence, and agency strategies as a combined management record. On that base it develops diagnostic tools that work without pretending that complex human systems reduce to one definitive score. Those tools are applied to case evidence from WFP, UNHCR, UNDP, UNICEF, WHO, and wider UN reform work, and the analysis is translated into recommendations for UN entities, country teams, donors, governing bodies, and UN-aligned partners.
The central research question is: how can strategic risk management improve United Nations system performance when crises are compound, authority is distributed, and results are politically and ethically consequential? Five subsidiary questions follow. How should risk leadership differ from ordinary enterprise risk management? Which capabilities allow foresight and risk sensing to alter budgets, decision rights, and partner arrangements? How can results-based management be strengthened by risk adjustment? What do selected UN cases reveal about execution under pressure? Which diagnostic tools can support management learning without creating false precision?
The stance taken here is reform-minded but disciplined. It rejects two weak positions: romantic multilateralism, which praises cooperation while ignoring institutional constraints, and cynical reductionism, which treats the UN only as bureaucracy. A serious analysis must hold both truths. The UN system carries urgent mandates and also operates through budgets, committees, procurement, staff safety systems, data platforms, reporting cycles, country teams, donors, and accountability mechanisms. The credibility of strategy depends on what happens inside those mechanisms.
1.3 Significance of the Study
The subject matters because the legitimacy of multilateral action is increasingly tied to delivery under stress. Member states and communities do not only ask whether a mandate is noble. They ask whether the institution can deliver when funds fall short, access closes, data fail, political conditions shift, or public trust weakens. Humanitarian need continues to rise while resources are strained. Development gains are repeatedly threatened by climate shocks, conflict, debt, and public health emergencies. Digital tools create new possibilities, but also new forms of exclusion, bias, surveillance risk, and institutional dependency.
For UN managers, the paper offers a way to test whether risk management is changing choices or merely producing documents. For donors and governing bodies, it offers a more exact oversight vocabulary than simply asking for more reporting. For UN-facing partners, it clarifies what credible alignment requires: governance readiness, safeguards, data responsibility, financial discipline, partner support, evaluation follow-up, and the courage to report difficulty before failure becomes public. For academic readers, it links risk governance, public management, humanitarian operations, strategic foresight, resilience, evaluation, and technology governance in one applied frame.
The central practical value of the study is its insistence on answerability. A strategically risk-informed institution should be able to say what risk was seen, who saw it, who had authority to respond, what changed, what resource moved, what safeguard was activated, which affected population was consulted, what result survived, and what was learned. That level of answerability is not an administrative luxury. In multilateral operations, it is part of mandate integrity.
Chapter 2: Evidence Base and Literature Review
The literature and policy base for the research is deliberately institutional and applied. The research is not building an abstract theory of risk detached from operational reality. It is examining how public organizations with complex mandates can convert uncertainty into better judgment. The evidence base therefore includes UN reform materials, enterprise risk management work, agency strategic plans, evaluation materials, results frameworks, business continuity and resilience sources, and selected public management concepts. The sources are read with caution. They are not treated as identical forms of evidence.
A policy brief or strategic plan shows what an institution intends to value. A results framework shows how it proposes to measure progress. A management plan shows how resources and functions are organized. An evaluation or oversight report often shows where the system actually struggles. A public case example may illustrate practice, but it rarely captures the internal decision sequence. This hierarchy matters. Doctoral work cannot simply place citations beside claims. It must examine what the citation can legitimately prove.
2.1 Strategic Risk Management in Multilateral Institutions
Enterprise risk management has matured across the UN system, and that is a meaningful development. The Joint Inspection Unit’s 2020 review of enterprise risk management in United Nations system organizations proposed updated benchmarks and emphasized integrated ERM as a basis for more proactive, better-informed decision-making, governance, oversight, and accountability (Joint Inspection Unit, 2020). This is a useful foundation, but it also reveals the key limitation. ERM can support strategy only when it is connected to planning, budgeting, programme review, partner management, and leadership forums.
Strategic risk management differs from ordinary operational control because it asks whether the organization can still deliver its mandate when major assumptions fail. A procurement delay, cybersecurity weakness, funding cut, access restriction, or partner capacity gap becomes strategic when it affects mandate delivery, protection, public trust, or institutional legitimacy. The same event may be routine in one context and strategic in another. A late shipment in a stable operation may be inconvenient; in a famine-risk operation it can become life-threatening.
Multilateral institutions also face a moral difference from many private organizations. A company may define risk through financial exposure, compliance exposure, market position, and reputation. A UN entity must also account for risks to people affected by action or inaction. Protection failure, exclusion, unsafe data collection, exploitation and abuse, inability to reach remote populations, and erosion of trust are not peripheral risks. They are part of the mandate environment. Risk appetite in such settings cannot be only technical. It must ask who bears the consequence if the risk materializes.
This is why risk leadership must be located above the register. A register records recognized risks; it does not prove that judgment changed. The stronger question is whether risk information enters the meeting where authority, money, staffing, and trade-offs are decided. In the UN context, that may mean country programme boards, humanitarian country teams, inter-agency coordination structures, senior management groups, donor consultations, procurement committees, data governance boards, or safeguarding review mechanisms. Risk that does not enter those forums remains administratively visible but strategically weak.
2.2 UN 2.0 and the Capability Shift
UN 2.0 is one of the most important contemporary sources for the research because it defines a capability agenda for a more demanding operating environment. The agenda emphasizes data, digital solutions, innovation, foresight, and behavioural science as a “quintet of change” intended to help the UN system become more agile, evidence-informed, and future-ready (United Nations, 2023). These capabilities have direct implications for risk management.
Data can improve early warning, targeting, monitoring, fraud detection, and resource allocation. But poor data can also create a false sense of precision. Digital tools can expand reach and reduce duplication. They can also exclude people without connectivity, increase cybersecurity exposure, or concentrate sensitive information. Innovation can improve delivery if it solves real field problems and scales responsibly. It can also produce pilot fatigue if incentives reward novelty more than adoption. Foresight can help leaders prepare for plausible futures, but only if it affects budget and decision rights. Behavioural science can improve programme design and public communication, but it requires ethical boundaries, especially where vulnerable populations are involved.
The promise of UN 2.0 is that reform is framed as capability rather than slogans. The risk is that capability language becomes another vocabulary layer. A UN entity may speak about foresight while budgeting remains too rigid to act on scenarios. It may speak about digital transformation while training, interoperability, accessibility, and privacy controls lag behind. It may celebrate innovation without building pathways for procurement, governance, scale, and evaluation. The research therefore treats UN 2.0 as both opportunity and test. The test is whether its capabilities alter decisions under pressure.
Strategic risk management can serve as the bridge. Risk sensing needs data. Risk anticipation needs foresight. Risk treatment needs innovation. Risk communication needs behavioural insight. Risk governance needs digital discipline. But each capability must be tied to authority and safeguards. Otherwise the organization becomes more informed without becoming more decisive, and more digitally ambitious without becoming more trusted.
2.3 The Pact for the Future and Duties to Tomorrow
The Pact for the Future, adopted by world leaders at the Summit of the Future on 22 September 2024, together with the Global Digital Compact and the Declaration on Future Generations, places reform of international cooperation in a broader political frame (United Nations, 2024). It is relevant here because it lengthens the accountability horizon. Institutions are not only being asked to deliver current outputs. They are being asked to consider how today’s decisions affect future generations, digital governance, peace, security, development, and global public goods.
Future orientation changes risk analysis. A choice that looks efficient in the short term may weaken resilience over time. Underfunding preparedness, neglecting climate adaptation, failing to protect education during crises, allowing debt distress to reduce social spending, or deploying digital systems without rights safeguards can defer harm rather than prevent it. Strategic risk management must therefore ask what harms are being postponed because current incentives make prevention politically invisible.
The Global Digital Compact also sharpens the technology dimension. Digital cooperation promises inclusion, data use, innovation, and AI governance, but the same tools can create exclusion, surveillance, dependency, and power asymmetry. A UN-facing risk framework must therefore require purpose limitation, privacy, cybersecurity, human oversight, bias review, grievance routes, and transparency before digital systems become operationally central. Technology risk cannot be handled after scale. It must be designed into the programme from the beginning.
A future generations lens also forces budget honesty. It is easy to speak for tomorrow while spending only for today. A serious future-oriented institution must identify which investments strengthen resilience across multiple futures: data quality, public health preparedness, climate adaptation, child protection systems, flexible finance, partner capacity, and institutional learning. Strategic risk management provides a method for translating future language into present controls.
2.4 Risk-Informed Development and the Humanitarian-Development-Peace Nexus
Risk-informed development is central to the argument because development gains can be erased by shocks if programmes are designed for stable assumptions. UNDP’s risk-informed development strategy tool emphasizes the integration of disaster risk reduction and climate change adaptation into development planning and investments, while also addressing policy silos and multidimensional risk (UNDP, 2021). That premise is especially important in countries where climate exposure, fragile governance, economic pressure, and social inequality interact.
The humanitarian-development-peace nexus is often discussed as coordination language, but it is also a risk-management problem. Humanitarian action may save lives immediately while development investment reduces future need. Peacebuilding may affect access, trust, and institutional resilience. Poorly coordinated interventions can create parallel systems, duplicate assessments, overload local partners, or weaken national ownership. A strategic risk lens asks which action reduces immediate harm, which strengthens systems, and which accidentally creates dependency or unmanaged exposure.
UNICEF’s strategic planning across successive cycles illustrates the same point from the perspective of children (UNICEF, 2021). Its 2026-2029 Strategic Plan describes a final drive toward child-related Sustainable Development Goals by 2030, with sharpened focus, differentiated strategies, agility, resources, partnerships, and a commitment to leaving no child behind (UNICEF, 2025). For children, risk is cumulative. A disruption in education, nutrition, health, protection, or social assistance can produce effects that last decades. Equity is therefore not a decorative factor in results. It determines whether the mandate is reaching those most likely to be harmed.
WFP’s strategic planning and corporate results work similarly links operational focus, programme quality, results measurement, and management enablers (WFP, 2022). Its 2026-2029 corporate results framework is explicitly designed to translate the strategic plan into implementation and measurement architecture (WFP, 2025a). The lesson is that risk management must enter the results architecture. It is not enough to know what will be delivered. Leaders must know what can prevent delivery, which groups may be missed, what quality standards must hold, and which residual risks remain after implementation.
2.5 Results-Based Management, Evaluation, and Learning
Results-based management is necessary for accountability, but it can become misleading if treated as mechanical reporting. The Joint Inspection Unit has described results-based management as a high-impact model for managing toward results across the UN system (Joint Inspection Unit, 2017). In principle, RBM links planning, implementation, monitoring, reporting, and learning. In practice, indicators can become separated from context. This is particularly dangerous in humanitarian, protection, and governance work, where numerical outputs may not capture whether people are safer, rights are protected, or institutions are more resilient.
UNHCR’s results work illustrates both the importance and the limits of consolidation. Public materials describe the use of core indicators to support global presentation of results across operations (UNHCR, 2025). That is necessary for a global organization. Yet protection outcomes depend on legal access, confidentiality, documentation, safe referral pathways, community trust, and political conditions. A core output indicator may be necessary, but it is not sufficient. Strategic risk management asks what the indicator does not show.
Evaluation is the corrective discipline. UNHCR’s evaluation strategy for 2024-2027 emphasizes evaluation as part of an organizational results-based management culture and practice, with credible evaluations used to demonstrate results and value for money (UNHCR, 2024). This is the right direction, but the managerial test is follow-up. An evaluation that identifies problems but does not alter budget, staffing, partner design, or leadership review becomes a form of institutional memory without institutional movement. For that reason, this research treats evaluation recommendations as risk signals that require owners, deadlines, and evidence of action.
Learning must also occur before the post-crisis review. Traditional evaluation cycles are often too slow for volatile contexts. Monitoring, community feedback, partner reporting, safeguarding data, and operational signals should provide live learning. The point is not to abandon formal evaluation. The point is to prevent evaluation from being the first moment at which the organization admits what field staff already knew.
2.6 Organizational Resilience, Efficiency, and Business Continuity
The United Nations Organizational Resilience Management System is relevant because strategic risk management is not only about external programmes. The institution itself must continue critical functions during disruption. CEB materials describe organizational resilience as a cross-functional endeavour involving crisis management, security, business continuity, ICT disaster recovery, medical emergency response, crisis communication, and support to staff, survivors, and families (United Nations System Chief Executives Board for Coordination, 2021). This is not a back-office issue. It is mandate protection.
Resilience should not mean asking staff and partners to absorb impossible pressure. An organization can appear resilient while transferring risk to local staff, underfunded partners, or affected communities. True resilience requires preparedness, clear authority, redundancy where necessary, trained crisis teams, duty-of-care arrangements, surge capacity, and business continuity plans that are tested rather than filed. If local partners carry delivery in insecure areas without adequate support, the system has not localized resilience; it has displaced risk.
Efficiency is equally complex. HLCM’s management reform work focuses on financial management, procurement, human resources, digitalization and technology, and safety and security, with recent efficiency initiatives addressing resource pressure and system-wide savings (United Nations System Chief Executives Board for Coordination, 2025). Efficiency can strengthen delivery when it reduces duplication, procurement friction, unnecessary reporting, or slow business processes. It can weaken resilience when it cuts protective capacity, removes redundancy, reduces oversight, or underfunds learning. The central question is not whether efficiency is good, but where savings come from and who carries the risk afterward.
Funding volatility cuts across all of this. Organizations facing unpredictable resources may delay commitments, reduce field presence, cut monitoring, stretch partner agreements, or prioritize activities that are easier to fund rather than those most strategically necessary. A risk-informed strategy must therefore treat finance as a delivery risk, not merely a resource variable. It should identify which commitments fail first under funding contraction, which populations lose support, which safeguards become exposed, and what contingency decisions are available.
2.7 Literature Gap
The reviewed materials provide strong components: UN 2.0 offers a capability agenda; the Pact for the Future offers political and temporal urgency; JIU enterprise risk management work offers system benchmarks; UNDP and UNICEF materials support risk-informed programming; WFP and UNHCR materials show results and operational dilemmas; WHO materials show the pressure of preparedness; CEB and ORMS materials show resilience and management reform. The gap is integration at the leadership level.
Leaders need a practical way to connect risk sensing, foresight, decision rights, resource mobility, safeguards, partner coordination, evidence learning, and results reporting. Many frameworks identify principles. Fewer show how a manager might diagnose delay, compare readiness across units, adjust results for risk, or test whether partnerships are carrying hidden exposure. This research addresses that gap through diagnostic models designed for management deliberation rather than statistical display.
Table 1. Strategic risk domains and leadership control questions
| Risk domain | Leadership question | Primary control evidence |
| Conflict and access risk | Can operations adapt when security, access, or political conditions change? | Scenario review, access protocols, partner contingency, security escalation |
| Climate and disaster risk | Are programmes designed for foreseeable environmental stress? | Climate risk screening, early warning, adaptation finance, continuity planning |
| Funding volatility | Which commitments fail first if resources contract? | Prioritization rules, flexible funding, donor dialogue, contingency budgets |
| Protection and safeguarding | Who is exposed to harm if controls fail? | Complaint pathways, survivor-centered response, partner training, incident follow-up |
| Data, digital, and AI risk | Can tools be explained, secured, challenged, and shut down if unsafe? | Data governance, privacy controls, cybersecurity, human oversight |
| Partner capacity risk | Are partners resourced to carry the responsibility assigned to them? | Payment timing, overhead, role clarity, dispute resolution, localization support |
| Trust and legitimacy risk | Can affected people and stakeholders see accountability? | Community feedback, public communication, evidence disclosure, grievance routes |
Chapter 3: Methodology and Diagnostic Model Design
The research uses an integrative documentary method. It analyzes public UN and UN-related materials, agency strategies, results frameworks, evaluation materials, oversight sources, and management reform documents, then translates them into diagnostic tools for strategic risk leadership. The method is appropriate because the object of analysis is not one programme in one country. It is the management problem that appears across multilateral operations: how to make risk information consequential.
The research does not claim statistical generalization. It does not use confidential interviews, internal dashboards, non-public risk registers, or proprietary UN data. That limitation is not hidden. It is central to the research design. Public institutional documents are not enough to prove implementation, but they are enough to analyze formal intent, stated governance expectations, management logic, and visible areas of operational concern. The value of the paper lies in disciplined synthesis and diagnostic design.
The research design follows four steps. It identifies the authoritative documents that shape the UN system’s current reform and risk environment, then classifies the evidentiary status of each source. From those sources it derives variables that recur across strategic risk, results, foresight, safeguards, partnership, and resilience materials, and converts those variables into models that leadership teams can use for structured review.
3.1 Source Selection and Evidence Handling
Documents were selected according to authority, relevance, recency, and operational usefulness. Official UN and agency sources are prioritized because the research is UN-facing. UN 2.0 and the Pact for the Future are used to establish current reform direction. JIU reports are used because they carry system-wide oversight value. Agency strategic plans and results frameworks are used to understand mandate translation and performance logic. Evaluation materials are used because they reveal learning expectations and organizational friction. CEB and ORMS materials are used to connect risk to business continuity and system management.
Evidence is handled conservatively. A strategic plan is not proof that implementation occurred. A public report is not proof that internal decisions were effective. An evaluation finding is not proof that all similar contexts share the same weakness. The analysis therefore avoids sweeping claims about the entire UN system unless supported by system-wide sources. Where the analysis makes an inference, it states the inference as such.
This is especially important for doctoral research because the temptation in institutional writing is to let official language do too much work. The existence of a policy does not prove risk maturity. The existence of a dashboard does not prove data quality. The existence of a partnership framework does not prove partner trust. The existence of an evaluation strategy does not prove learning. Each document is a clue to management design; it is not automatically evidence of management performance.
3.2 Model Design Principles
The diagnostic models are designed around five principles. They must be transparent, so a UN-facing manager can see the variables and debate them without needing a hidden algorithm. They must be adaptable, because a humanitarian logistics operation, a protection agency, a development programme, and a health emergency function will not weight every risk in the same way. They must be evidence-demanding, with scores supported by documents, field signals, partner feedback, incident data, decision records, and evaluation findings. They must be ethically alert, since a high delivery score cannot compensate for serious harm to affected populations. And they must expose delay, because risk intelligence has little value if the organization cannot act on it in time.
The models are therefore not presented as validated instruments. They are structured tools for leadership review. Their purpose is to improve questions, reveal assumptions, organize evidence, and make trade-offs visible. They should not be used to rank agencies publicly or punish units operating in severe contexts. A low score may indicate weak management; it may also indicate that a team is honest about extreme conditions. A high score may indicate maturity; it may also indicate optimism, weak evidence, or internal groupthink. The diagnostic conversation matters as much as the number.
3.3 Strategic Risk Leadership Index
The Strategic Risk Leadership Index, abbreviated SRLI, evaluates whether the organization has the leadership conditions needed to manage strategic risk. The proposed formula is:
SRLI = 0.14·MC + 0.13·RS + 0.12·FU + 0.12·DR + 0.11·RM + 0.10·PC + 0.10·EL + 0.10·SG + 0.08·ST − 0.10·DL
In the formula, MC is mandate clarity, RS is risk sensing, FU is foresight use, DR is decision rights, RM is resource mobility, PC is partner coordination, EL is evidence learning, SG is safeguards, ST is stakeholder trust, and DL is decision lag. Each component can be scored from zero to one hundred using evidence. The positive weights sum to 1.00, so the index behaves as a weighted average on a 0-100 scale before the decision-lag penalty is applied. The negative term for decision lag matters because an organization can possess strong policies, strong data, and strong language and still lose strategic value if action is too slow.
Mandate clarity asks whether broad mandates have been translated into priorities that can guide trade-offs. Risk sensing asks whether weak signals move from field teams, partners, affected communities, digital systems, security staff, procurement, and finance into leadership review. Foresight use asks whether scenarios affect decisions rather than remaining reflective exercises. Decision rights ask whether authority is clear and proportionate. Resource mobility asks whether money, people, supplies, or technical support can move when risk changes. Partner coordination asks whether roles are realistic and supported. Evidence learning asks whether monitoring and evaluation alter practice. Safeguards ask whether protection, rights, integrity, and data controls are active. Stakeholder trust asks whether affected people and partners can see accountability. Decision lag measures how long the system takes to respond.
A leadership team should not score the SRLI alone. The model should be used with cross-functional participation. A senior manager may believe decision rights are clear while field staff experience them as vague. A risk officer may view safeguards as strong while local partners experience them as underfunded. A data team may believe a platform is reliable while protection staff see privacy concerns. Differences in scoring are valuable because they reveal institutional blind spots. Figure 1 summarizes the relative weight the index assigns to each component.
Table 2. Strategic Risk Leadership Index components
| Component | Symbol | Weight | Leadership meaning | Evidence to request |
| Mandate clarity | MC | .14 | Mandate is translated into priorities and trade-off rules. | Strategic plan, country priorities, decision memos |
| Risk sensing | RS | .13 | Early signals reach leadership from field, partners, communities, and systems. | Early warning, partner feedback, incident logs, monitoring data |
| Foresight use | FU | .12 | Scenario thinking affects budget, staffing, procurement, and advocacy. | Scenario notes, budget triggers, contingency decisions |
| Decision rights | DR | .12 | Authority is clear, proportionate, and close enough to evidence. | Delegations of authority, escalation routes, approval timelines |
| Resource mobility | RM | .11 | Funds, people, supplies, or support can move as risk changes. | Flexible finance, surge rosters, budget revision records |
| Partner coordination | PC | .10 | Partners have roles, resources, safeguards, and realistic obligations. | Agreements, payment timing, role maps, partner assessments |
| Evidence learning | EL | .10 | Monitoring and evaluation change practice. | Management responses, implementation trackers, learning notes |
| Safeguards | SG | .10 | Protection, rights, integrity, and data controls are active. | Complaint data, safeguarding pathways, data protection review |
| Stakeholder trust | ST | .08 | Affected people and partners can see accountability. | Feedback systems, public claims evidence, survey results |
| Decision lag | DL | -.10 | Delay reduces risk leadership when signals do not become action. | Elapsed days from signal to response |
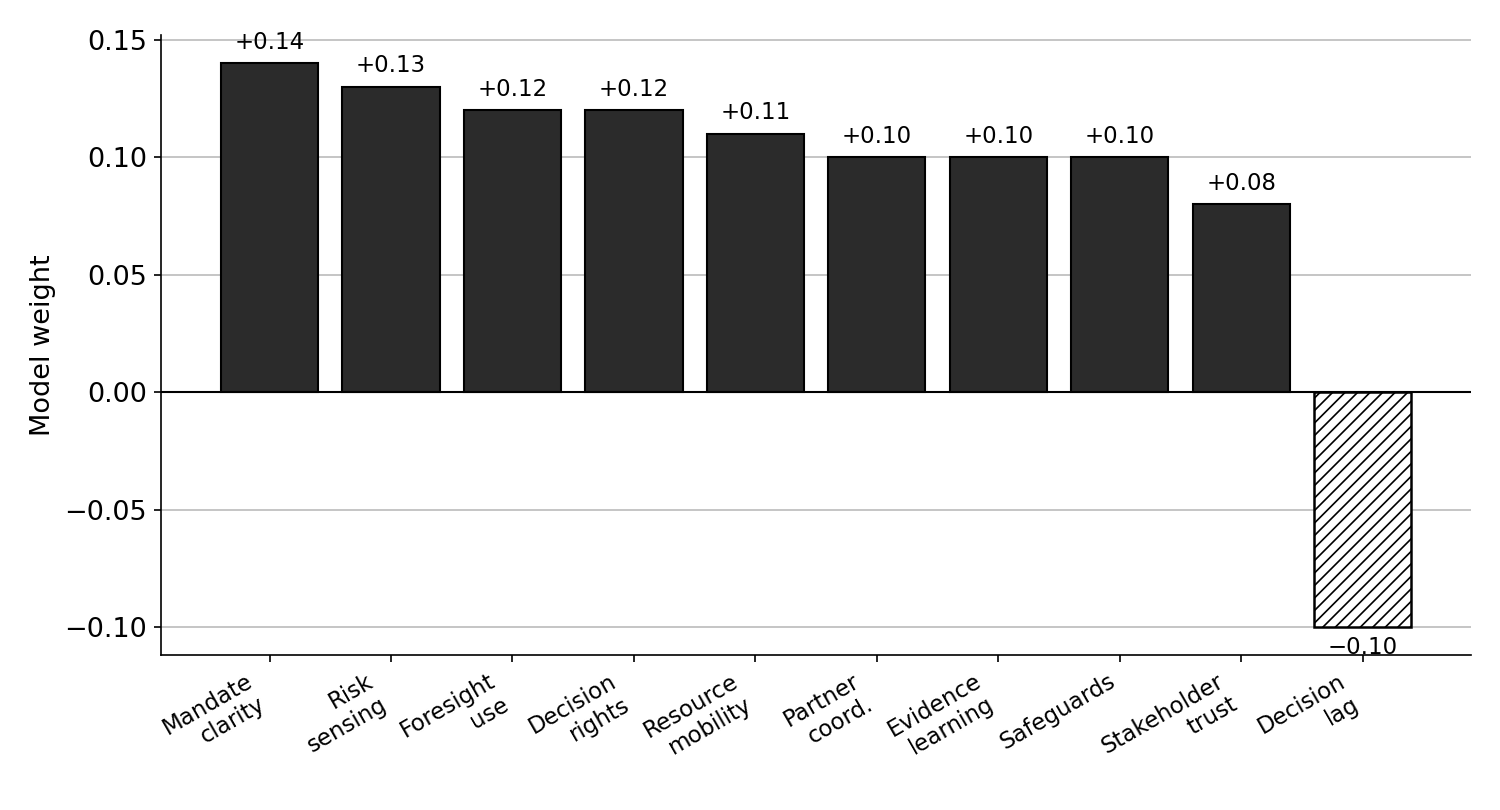
Figure 1. Strategic Risk Leadership Index: component weights.
3.4 Risk-Adjusted Results Delivery
The Risk-Adjusted Results Delivery model, abbreviated RARD, tests whether reported results remain credible once quality, equity, sustainability, residual risk, and harm are considered. The formula is:
RARD = (Results Delivered × Quality Factor × Equity Factor × Sustainability Factor) − Residual Risk Exposure − Harm Penalty
The model protects against false success. A programme may deliver a high number of outputs while excluding the hardest-to-reach populations, weakening local systems, or leaving serious protection concerns unresolved. Another programme may deliver fewer outputs but achieve higher strategic value because it reaches high-risk groups, strengthens national capacity, and reduces future exposure. The RARD model therefore invites leaders to examine not only how much was done, but what kind of result was produced.
The Quality Factor asks whether the result met required standards. The Equity Factor asks whether marginalized populations were reached. The Sustainability Factor asks whether the result can persist or whether it depends entirely on temporary external capacity. Residual Risk Exposure captures significant risks left unresolved after delivery. The Harm Penalty captures safeguarding failures, rights violations, data misuse, exclusion, or serious unintended consequences. In UN contexts, harm cannot be treated as a minor adjustment. Severe harm may invalidate otherwise impressive delivery numbers.
The model is useful for donor and governing body dialogue because it makes reporting more honest without making it cynical. It allows organizations to say: here is what we delivered, here is what held, here is who was missed, here is what remains fragile, here is the safeguard we activated, and here is what we will change. That form of reporting is more credible than polished success claims that hide unresolved exposure.
3.5 Decision-Lag Diagnostic
The Decision-Lag Diagnostic, abbreviated DLD, measures the time between risk signal and meaningful action. It is expressed as:
DLD = Signal Recognition Time + Risk Analysis Time + Approval Time + Resource Release Time + Partner Alignment Time + Field Start Time + Feedback Review Time
The score can be measured in days or weeks depending on the process. The diagnostic does not assume that speed is always good. Some decisions require careful review, especially where protection, legal exposure, security, fiduciary risk, or rights concerns are serious. The question is which delays are necessary and which are avoidable. A mature system should know the difference.
A long signal-recognition period suggests weak field intelligence or poor listening to partners and communities. A long analysis period may indicate fragmented data or unclear risk methodology. A long approval period may suggest excessive centralization or political sensitivity. A long resource-release period points to budget rigidity. A long partner-alignment period may reveal weak role clarity or unrealistic partnership design. A long field-start period may indicate procurement, staffing, security, or logistics barriers. A long feedback-review period suggests that learning is not institutionalized.
The DLD is especially important because delay is often invisible in final reporting. A report may say that assistance was delivered, but not that the risk was known weeks earlier. It may say a policy changed, but not that field staff had warned of the problem months before. By making time visible, the diagnostic turns delay into a management object. Figure 3 illustrates how a single decision can accumulate lag across the seven stages.
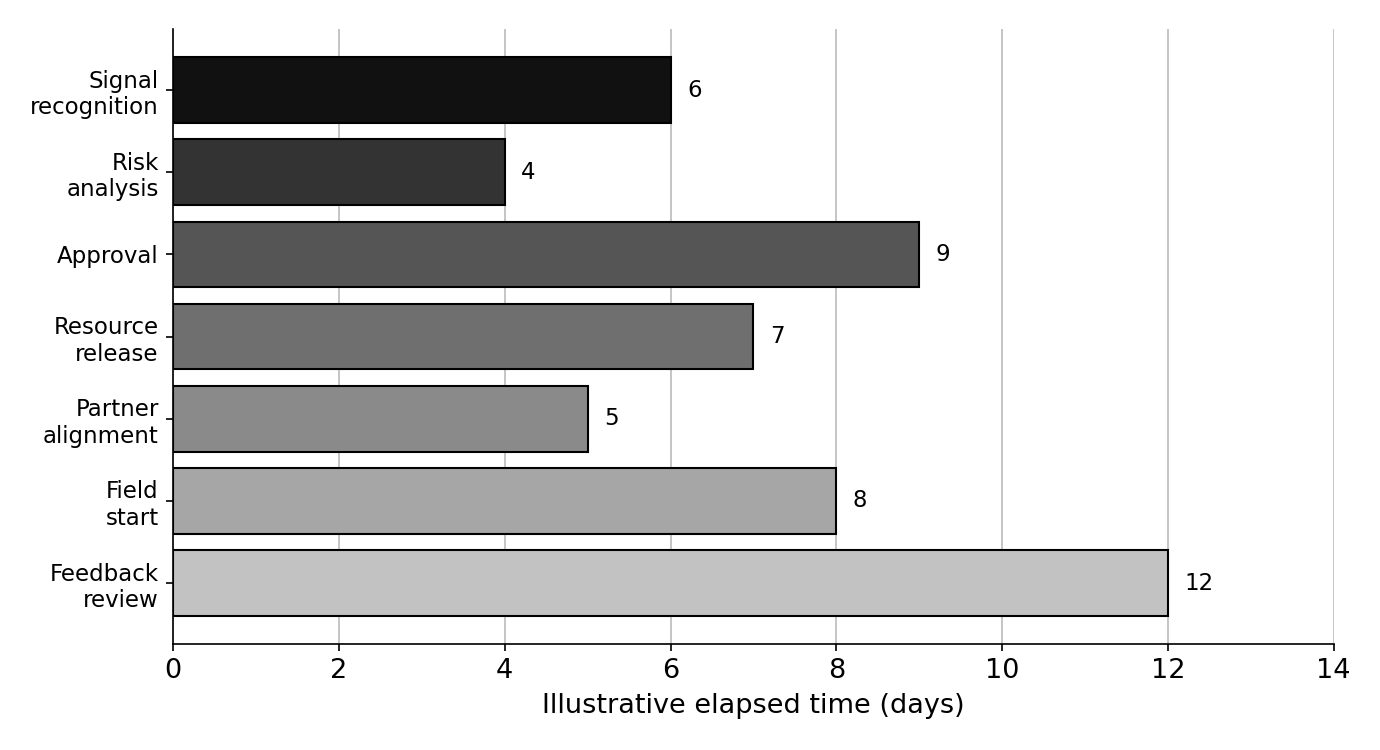
Figure 3. Decision-Lag Diagnostic: illustrative elapsed time across the seven stages.
3.6 Partner Trust and Accountability Score
The Partner Trust and Accountability Score, abbreviated PTAS, responds to a central multilateral reality: the UN system delivers through partnerships. Trust is not sentiment. In complex programmes, it is an operating condition. If roles are unclear, funding arrives late, reporting demands are disproportionate, safeguarding expectations are unfunded, data-sharing rules are ambiguous, or dispute routes are weak, the partnership becomes fragile.
The proposed formula is:
PTAS = 0.18·Transparency + 0.16·Role Clarity + 0.14·Safeguards + 0.13·Funding Reliability + 0.12·Data Sharing + 0.10·Feedback Loop + 0.09·Local Ownership + 0.08·Dispute Resolution
The eight positive weights again sum to 1.00, so the score reads on the same 0-100 scale as the other indices. It can be used by UN entities, donors, and partner organizations before scale. A partnership with weak role clarity, late payments, unclear data rights, and no credible dispute route should not be expected to carry high-risk delivery without redesign. Localization should strengthen local agency. It should not move risk downward while authority remains upward.
PTAS is also useful because it forces discussion of power. Large institutions may describe partnership positively while imposing terms that smaller organizations cannot absorb. Local partners may accept unrealistic obligations because funding options are limited. A risk-informed partnership asks who bears security risk, cash-flow risk, safeguarding risk, data risk, and reputational risk. If the answer is hidden, the partnership is not yet accountable. Figure 2 shows the relative weight of each PTAS component.
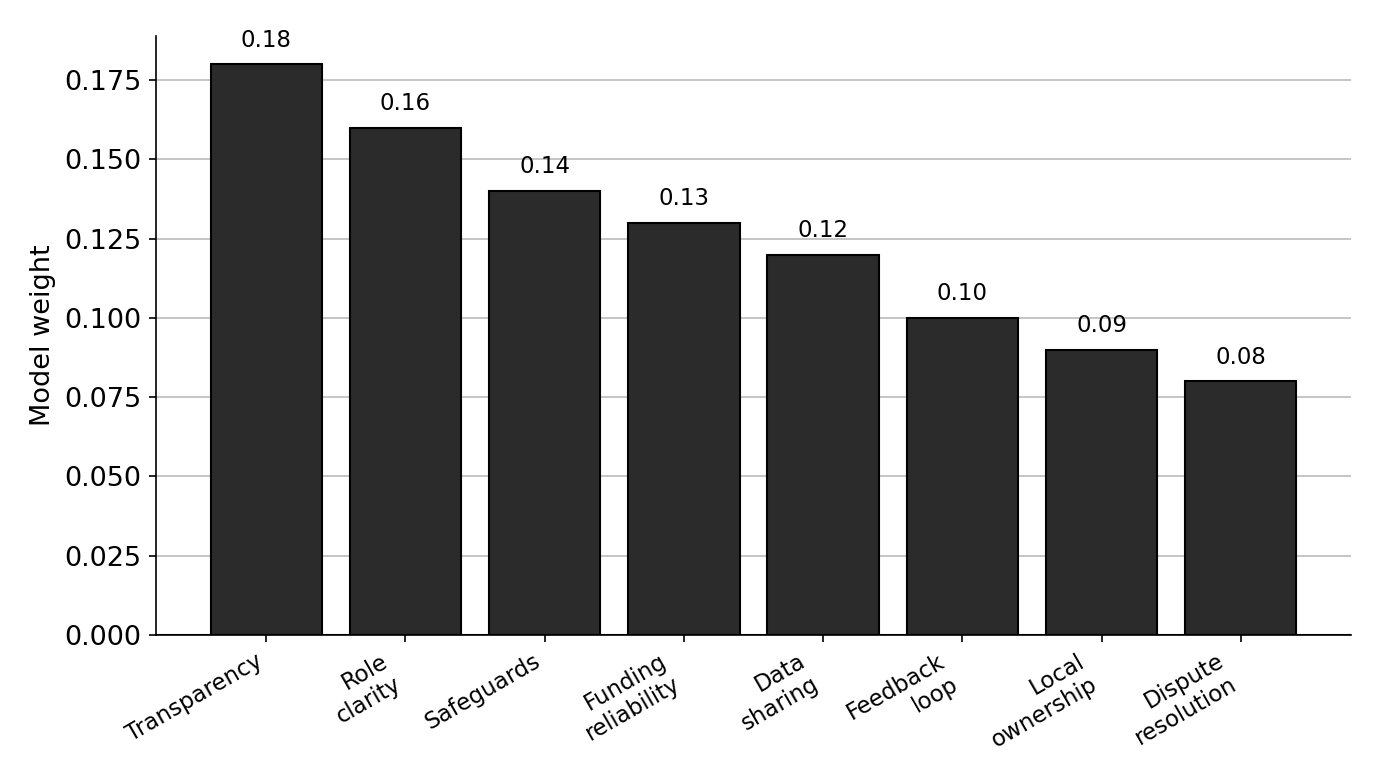
Figure 2. Partner Trust and Accountability Score: component weights.
3.7 Scenario Stress Test
The Scenario Stress Test asks a leadership team to examine whether a programme or strategy can survive plausible disruption. The team selects a programme and tests it against four shocks: funding contraction, access deterioration, data failure, and legitimacy shock. For each shock, the team asks what stops, what continues, who decides, which partners absorb burden, which affected groups are harmed first, what safeguard activates, and how the organization communicates.
The stress test is deliberately simple. It does not require advanced simulation to be useful. Its value lies in exposing fragile assumptions before the crisis exposes them. A programme that cannot identify what would continue after a moderate funding cut is not financially resilient. A programme with no safe alternative if access deteriorates is not operationally resilient. A programme dependent on one data platform is not digitally resilient. A programme with no credible response to public distrust is not legitimacy-resilient.
Stress testing also creates a practical bridge between foresight and management. Foresight often fails because it remains at the level of broad scenarios. Stress testing asks what those scenarios mean for budget, authority, partners, data, safeguards, and communication. It forces strategy to confront operating conditions.
Chapter 4: United Nations Case Readings
The case readings are not presented as audits. They are public-source management readings of selected UN entities and system-wide agendas. Each case is chosen because it exposes a different strategic risk dilemma. WFP illustrates hunger, supply chains, funding pressure, prioritization, and innovation discipline. UNHCR illustrates displacement, protection, global results, and evaluation follow-up. UNDP illustrates risk-informed development, national systems, and governance. UNICEF illustrates child-focused systems, equity, and intergenerational risk. WHO illustrates health emergency preparedness, trust, and financing volatility. UN 2.0 and the Pact for the Future illustrate system-wide reform.
The purpose is not to rank agencies. Different mandates require different capabilities. The purpose is to identify transferable leadership lessons.
4.1 WFP: Emergency Scale, Prioritization, and the Funding Cliff
WFP’s strategic risk environment is concrete and unforgiving. If supply routes fail, if funding drops, if access is blocked, if targeting data are weak, or if partners are overwhelmed, people may not eat. The risk profile therefore combines operational logistics, humanitarian access, donor volatility, nutrition, cash assistance, supply chains, local markets, protection, and public trust. WFP’s planning for 2026-2029 and corporate results work emphasizes strategic outcomes, cross-cutting priorities, enablers, and metrics that link corporate performance to programme delivery (WFP, 2025c). The key lesson is that results architecture and risk architecture must be integrated.
The first leadership dilemma is prioritization. When need exceeds resources, an organization cannot protect every commitment equally. The strategic question becomes: which capability must be defended because it carries the organization’s comparative advantage? For WFP, emergency food assistance, logistics, supply-chain capacity, vulnerability analysis, nutrition support, and field reach are not ordinary functions. They are core mandate assets. Risk management should help preserve them under stress.
The second dilemma is targeting and trust. Food assistance decisions can become politically and socially sensitive because inclusion and exclusion have immediate consequences. If vulnerability data are incomplete, if community feedback is weak, or if prioritization criteria are not understood, trust can deteriorate. Risk-adjusted results are essential here. Reporting the number of people reached matters, but it does not answer whether the right people were reached, whether rations were adequate, whether exclusions were justified, or whether community trust survived.
The third dilemma is innovation. WFP’s innovation strategy describes innovation in terms of impact at scale, field capacity, collaboration, and sustainable funding (WFP, 2025b). That is the right test. Humanitarian innovation should not be judged by novelty. It should be judged by whether it improves speed, targeting, safety, cost, accountability, or resilience without creating new harms. A digital targeting tool that increases efficiency but cannot be explained to communities may create legitimacy risk. A financing mechanism that accelerates assistance but shifts cash-flow exposure to local partners may weaken delivery. Innovation must therefore be governed as a risk-sensitive operating capability.
4.2 UNHCR: Protection, Displacement, and Results Integrity
UNHCR operates where strategic risk is inseparable from legal and human protection. Forced displacement intersects with conflict, statelessness, asylum systems, border politics, shelter, education, livelihoods, host-community pressure, climate stress, gender-based violence, documentation, and data confidentiality. The agency’s results materials emphasize global indicators and the presentation of results across operations (UNHCR, 2025). That global consolidation is necessary, but protection work cannot be reduced to output counts.
The first leadership dilemma is the relationship between numbers and protection meaning. Registering people, delivering assistance, supporting education, or providing shelter can be counted. Whether people are safer, whether legal pathways are credible, whether confidentiality is protected, whether community feedback is trusted, and whether durable solutions are realistic require deeper interpretation. Strategic risk management therefore requires protection risk analysis alongside quantitative results.
The second dilemma is evaluation follow-up. UNHCR’s evaluation strategy emphasizes the integration of evaluation into results-based management culture and practice (UNHCR, 2024). That aspiration is important because displacement operations often occur amid staff rotation, donor pressure, and urgent need. Institutional learning can easily be lost. A strategic risk system should treat evaluation recommendations as management signals with owners, resources, deadlines, and follow-up evidence. Without that chain, evaluation becomes a record of insight rather than a driver of change.
The third dilemma is data responsibility. Displacement data can be highly sensitive. Digital systems may improve registration and service delivery, but they also raise privacy, consent, protection, and cybersecurity concerns. In refugee and statelessness contexts, data misuse can create severe harm. Risk leadership must therefore insist on governance before scale: purpose limitation, data minimization, protection analysis, human oversight, grievance routes, and clear rules for sharing.
4.3 UNDP: Risk-Informed Development and National Systems
UNDP’s case illustrates the problem of risk that hides in time. A development programme may look successful during implementation and fail later when climate shock, fiscal distress, governance weakness, conflict, or institutional turnover returns. Risk-informed development asks whether the investment will still protect people when conditions change. UNDP’s risk-informed development materials emphasize integration of disaster and climate risks into development planning and investments, overcoming policy silos, and recognizing multidimensional risk (UNDP, 2021). That approach is central to resilient development.
The first leadership dilemma is systems strengthening versus project delivery. Development agencies are under pressure to show deliverables, but lasting value often comes from strengthening national systems: public finance, social protection, local governance, climate planning, data capacity, rule-of-law institutions, and service delivery. These results are harder to attribute and slower to show. Risk-adjusted reporting should therefore value institutional resilience, not only project outputs.
The second dilemma is national ownership under constraint. National ownership is essential, but institutions vary in capacity, legitimacy, and resources. A programme can be nationally aligned and still be fragile if public administration cannot maintain it, if recurrent financing is absent, or if political turnover changes priorities. Strategic risk management should ask whether the programme depends on temporary external capacity, whether domestic financing is plausible, and whether local actors can maintain the result.
The third dilemma is cross-sector risk. Climate adaptation, governance, digital public infrastructure, social protection, energy transition, and poverty reduction do not sit in separate risk lanes. They interact. A digital identity system may improve social protection targeting and raise data protection risks. Climate finance may build resilience or reinforce elite capture. Governance reform may improve service delivery or create political backlash. UNDP’s strategic value lies partly in helping countries see these interactions before programmes harden into silos.
4.4 UNICEF: Equity, Child Systems, and Intergenerational Risk
UNICEF’s mandate makes intergenerational risk concrete. Children experience institutional failure through lost learning, malnutrition, preventable disease, violence, displacement, unsafe water, mental health harm, and exclusion from social protection. The UNICEF Strategic Plan 2026-2029 is framed as the organization’s final drive toward child-related SDGs before 2030, with emphasis on focus, agility, resources, partnerships, and children’s rights (UNICEF, 2025). The strategic risk question is whether systems can protect children when crises overlap.
The first leadership dilemma is equity. A programme may reach large numbers while missing children with disabilities, girls in insecure regions, refugee and migrant children, children outside school systems, or children in communities beyond government reach. For UNICEF, equity is not a moral appendix to results; it is the condition that gives results mandate value. The RARD model therefore gives equity a central place.
The second dilemma is systems versus emergency delivery. Humanitarian action for children often requires immediate service provision. Longer-term child outcomes require resilient health, education, nutrition, WASH, protection, and social protection systems. If emergency delivery bypasses national and local systems without a transition plan, it may save lives now while weakening future resilience. If system strengthening moves too slowly during crisis, children suffer immediate harm. Strategic risk leadership lies in balancing the two without pretending that one can replace the other.
The third dilemma is voice and accountability. Children and young people are not merely beneficiaries. They are rights holders. A child-sensitive risk framework should ask whether programmes hear children safely, whether complaint pathways are accessible, whether data collection protects them, and whether decisions account for long-term consequences. Future generations language becomes real only when today’s systems are accountable to children now.
4.5 WHO: Preparedness, Health Emergencies, and Trust
WHO’s emergency role shows why preparedness is a strategic risk discipline. Health emergencies are system shocks. They affect economies, education, trust, mobility, public finance, and political stability. WHO’s 2025 health emergency materials describe an unprecedented convergence of health threats driven by conflict, climate change, food insecurity, antimicrobial resistance, and outbreaks, while emphasizing the need to protect lives from health emergencies (WHO, 2025a), and its emergency appeal sets out the financing required to meet that need (WHO, 2025b). The strategic risk problem is that preparedness is often underfunded until an emergency becomes visible.
The first leadership dilemma is prevention versus response. Emergency response attracts urgency because harm is visible. Preparedness competes for attention because success often means a crisis did not occur or did not escalate. Strategic risk management must make preparedness visible in results terms: surveillance capacity, trained personnel, supply readiness, legal frameworks, laboratory systems, risk communication, community engagement, and financing mechanisms.
The second dilemma is trust. Public health guidance can be technically accurate and still fail if communities distrust authorities or misinformation spreads faster than reliable communication. UN 2.0’s behavioural science capability matters here, but only with ethical discipline. Risk communication is not public relations. It is part of the intervention. It must listen, adapt, disclose uncertainty, and work through trusted local actors.
The third dilemma is financing. WHO’s emergency appeals and programme reports repeatedly show the pressure created by insufficient flexible funding. When emergency functions rely heavily on voluntary and earmarked resources, preparedness and core capacity are exposed. Strategic risk leadership should therefore treat flexible financing as a health security control, not a mere administrative preference.
4.6 UN 2.0 and the Pact for the Future as System-Wide Cases
UN 2.0 and the Pact for the Future can be read as system-wide cases because they are not agency strategies. They are attempts to shift the capacity and legitimacy of multilateral cooperation. UN 2.0 asks whether the UN system can become stronger in data, digital tools, innovation, foresight, and behavioural science. The Pact asks whether global cooperation can become more inclusive, effective, future-oriented, and able to address digital governance and intergenerational responsibility.
The strategic risk is breadth. When everything matters, priority can dissolve. A system-wide reform agenda succeeds only when translated into operational decisions. What does UN 2.0 mean for a country office’s next planning cycle? What does the Pact mean for a budget decision? Which digital compact commitments affect beneficiary data systems? Which future generations commitments affect climate adaptation, education, health preparedness, and procurement? Which foresight outputs trigger resource movement?
The diagnostic tools in this research offer one translation mechanism. They do not solve the politics of multilateral reform, but they help prevent broad agendas from floating above management reality. They ask whether capability becomes authority, whether foresight becomes budget, whether digital ambition becomes governance, whether partnership becomes shared accountability, and whether results survive risk-adjusted scrutiny.
Table 3. Case-study matrix
| Case | Strategic risk dilemma | Leadership lesson |
| WFP | Hunger risk, supply chains, targeting, funding contraction, innovation discipline | Protect comparative advantage while making prioritization and targeting accountable. |
| UNHCR | Displacement, protection, legal status, confidentiality, global indicators | Attach results to protection meaning, data responsibility, and evaluation follow-up. |
| UNDP | Development investments exposed to climate, fiscal, governance, and institutional risk | Risk-proof development by strengthening national systems and testing sustainability. |
| UNICEF | Child outcomes shaped by equity, systems, emergencies, and intergenerational harm | Treat equity and long-term opportunity as central results conditions. |
| WHO | Preparedness underfunded until crisis; trust and misinformation shape response | Make preparedness, risk communication, and flexible financing visible as controls. |
| UN 2.0 / Pact | Broad reform agendas risk weak translation into field decisions | Tie capability and future commitments to budget, authority, safeguards, and learning. |
Chapter 5: Strategic Risk Leadership Analysis
Across the evidence and cases, a consistent pattern appears. Strategic risk management succeeds when leaders can turn weak signals into timely, defensible choices without losing safeguards, trust, or results discipline. It fails when risk is documented but not acted upon, when foresight is not connected to budget, when results are reported without risk context, when efficiency hides risk transfer, or when digital ambition outruns governance.
This chapter moves from case description to leadership analysis. It identifies the core leadership practices that separate risk-aware organizations from risk-informed organizations.
5.1 Risk Is a Leadership Signal Before It Is a Register Entry
Risk registers have value, but they can create a false sense of control. A register proves that a risk has been named. It does not prove that the organization changed course. In complex institutions, a risk can be recorded, reported, and archived while the programme continues as if nothing changed. Strategic risk leadership begins when risk information reaches a forum where choices can be made.
Field offices often see risk first. Local partners may detect community dissatisfaction before surveys do. Protection staff may observe patterns before complaints rise. Procurement officers may notice supplier fragility before programme delays appear. Security staff may recognize access deterioration before programme teams revise targets. Data officers may see privacy and cybersecurity exposure before senior managers understand the delivery implications. A mature organization treats these signals as assets rather than disruptions.
The cultural issue is decisive. If bad news is punished, delayed, or softened, the organization will be late. If risk escalation is treated as disloyalty, field intelligence will become less honest. If senior leaders prefer polished dashboards to difficult narratives, the risk system will produce comfort rather than truth. Strategic risk management therefore requires psychological and institutional safety for escalation. People must be able to say, “the assumption is failing,” without fearing that the warning itself will be treated as failure.
Risk sensing also requires diversity of sources. A dashboard may show trends, but it may miss informal exclusion, fear, stigma, or community anger. A partner report may show delivery, but not the strain under which delivery occurred. A complaint mechanism may show few complaints because people trust the programme, or because they do not believe complaining is safe. Risk leadership asks what the data cannot see.
5.2 Foresight Must Affect Budget and Authority
Foresight is attractive because it signals sophistication. Its real test is whether it changes resource decisions. A scenario exercise that identifies likely climate stress, conflict spillover, funding contraction, or digital exposure but leaves budgets unchanged has not improved strategic readiness. It has improved institutional vocabulary.
For UN-facing organizations, foresight should trigger practical options: contingency budgets, pre-positioned supplies, surge rosters, partner framework agreements, data backup arrangements, risk communication plans, or donor discussions about adaptive funding. A scenario without a resource option is a conversation. A foresight function without access to decision forums will remain advisory at best and decorative at worst.
The Pact for the Future intensifies this point. Future generations cannot be protected by declarations alone. A future-oriented institution must ask whether current spending and management choices are creating resilience that future communities will inherit. Preparedness, climate adaptation, education continuity, child protection systems, health surveillance, cybersecurity, and local partner capacity are not secondary investments. They are the infrastructure of future risk reduction.
Foresight also requires humility. It is not prediction. It is disciplined rehearsal. Its strongest value is identifying choices that remain sensible across several plausible futures. Stronger data quality, clearer escalation routes, flexible finance, partner support, safeguarding capacity, and institutional learning are useful across many scenarios. These are resilience investments, even when they are politically less visible than crisis response.
5.3 Decision Rights Determine Whether Intelligence Becomes Action
Risk intelligence is wasted when no one knows who can act. Large systems often generate delay through structural ambiguity. A country office may understand the risk but lack budget authority. A regional bureau may agree but need headquarters approval. A donor may hold the key flexibility. A partner may know the local reality but lack authority to change the workplan. The result is not ignorance; it is immobilized knowledge.
Decision rights must be proportionate. Not every decision belongs at headquarters. Reversible operational decisions should often sit close to the evidence. Irreversible decisions, high protection risks, major financial exposure, significant reputational risk, or politically sensitive choices require higher review. A mature risk system does not centralize everything in the name of control. It defines control through clarity, proportionality, and escalation discipline.
Decision rights must also be visible before crisis. A team should know who can suspend a data tool, approve a budget reallocation, change targeting criteria, escalate a safeguarding concern, activate a security protocol, or revise a partner agreement. If authority is discovered during the crisis, delay has already entered the system.
The Decision-Lag Diagnostic helps by breaking delay into parts. Some delay protects quality. Some protects habit. Some protects nobody. Measuring the stages allows leaders to distinguish careful review from bureaucratic drift. The goal is not speed at any cost. The goal is timely judgment with safeguards intact.
5.4 Risk Appetite Must Be Ethical
Risk appetite is difficult in UN work because the organization is rarely taking risk only on its own behalf. It may be taking risk on behalf of affected populations, staff, local partners, donors, host governments, and future communities. A humanitarian organization may accept security risk to reach people in need, but it cannot casually move that risk to local staff without duty-of-care support. A development agency may pilot a digital tool, but it cannot treat vulnerable communities as test subjects without consent, safeguards, and accountability.
A technical risk appetite statement may classify tolerances as high, medium, or low. That is useful, but incomplete. Ethical risk appetite asks who bears the consequence if the risk materializes. It asks whether affected people were consulted. It asks whether partners have the resources to comply with standards. It asks whether urgency is being used to excuse weak controls. It asks whether a decision would remain defensible if the trade-off became public.
This ethical dimension distinguishes UN-facing risk leadership from many corporate settings. The goal is not simply to protect institutional assets. It is to protect mandate integrity, people, rights, staff, partners, public trust, and the credibility of international cooperation. Sometimes the ethical choice is to accept operational risk because inaction would be worse. Sometimes the ethical choice is to refuse scale because safeguards are not ready. The discipline is to make the trade-off explicit rather than hiding it behind neutral language.
5.5 Results Must Be Read With Risk Attached
Results without risk context can flatter institutions. A programme may deliver a large number of outputs while leaving serious vulnerabilities unresolved. A cash programme may reach households while increasing protection risks for women in a particular context. A digital registration process may improve speed while excluding people without identity documents. A training programme may report attendance while systems remain unable to sustain practice. Risk-adjusted interpretation prevents success claims from becoming detached from reality.
The pressure to report scale is understandable. Donors, governing bodies, and the public often ask how many people were reached. That question matters, but it is not enough. Leaders also need to know who was not reached, whether the result met standards, whether the outcome can survive, whether local systems were strengthened, and whether harm occurred. The RARD model exists to make those questions normal.
Risk-adjusted results are also fairer to field teams. Delivering an output in a remote, insecure, climate-affected area with weak infrastructure and distrust is not the same as delivering the same output in a stable capital. A system that treats both outputs as equal may unintentionally reward easy delivery and punish difficult mandate work. Strategic risk management should make the difficult result visible.
This does not mean turning every report into a catalogue of problems. It means making reporting more credible. A mature report can say: these results were achieved; this is the quality evidence; these groups were reached and missed; this risk was reduced; this residual exposure remains; these safeguards worked; these harms or complaints were addressed; this is how the next cycle will change. Such reporting builds trust because it admits complexity without surrendering accountability.
5.6 Partner Coordination Is a Risk Control
Partnership is often described as a value. It is also a control. No UN agency delivers alone. Governments, local civil society, international NGOs, private suppliers, community groups, donors, and other UN entities all shape outcomes. When partnership design is weak, risk multiplies: unclear roles, duplicate reporting, payment delay, safeguarding gaps, data confusion, procurement disputes, community mixed messages, and accountability gaps.
Local partners are often closest to risk. They may know which families are excluded, which community leaders are trusted, which routes are unsafe, which grievance channels are feared, and which programme assumptions are unrealistic. But proximity to risk does not mean capacity to absorb risk. If local partners are underfunded, undertrained, paid late, or overloaded with reporting, the system is using their courage as a substitute for management.
The PTAS model therefore treats partnership quality as a strategic issue. Transparency, role clarity, safeguards, funding reliability, data-sharing rules, feedback loops, local ownership, and dispute resolution determine whether a partnership can carry pressure. A partner that cannot challenge unrealistic timelines will not be able to prevent failure. A partner that lacks overhead cannot build the systems required for accountability. A partner that is expected to carry security risk without support is being used, not localized.
Strategic risk leadership should map risk allocation across the partnership. Who carries fiduciary risk? Who carries staff safety risk? Who carries safeguarding risk? Who carries data risk? Who carries public blame if delivery fails? If authority and risk are separated too sharply, partnership becomes unstable.
5.7 Data, Digital, and AI Require Governance Before Scale
The UN system’s data and digital capabilities are expanding, and the potential value is substantial. Better data can improve early warning, targeting, supply planning, fraud detection, programme adaptation, translation, and monitoring. Digital platforms can reduce duplication and expand reach. AI can support pattern recognition, triage, analysis, and communication. Yet each benefit carries risk. The most dangerous digital systems are not always the ones that fail completely. They are the ones that work well enough to be trusted while carrying bias, exclusion, privacy exposure, or false certainty.
A UN-facing digital risk discipline should include purpose definition, data minimization, consent or lawful basis, privacy review, cybersecurity, bias assessment, interoperability, accessibility, human oversight, model monitoring, grievance routes, and shutdown conditions. These questions must be asked before scale, not after. A system that cannot be explained to staff or affected communities is not ready for sensitive deployment.
AI raises additional concerns. Models can reproduce bias, obscure accountability, produce plausible errors, or shift decision-making away from human judgment. In humanitarian and rights-sensitive settings, AI should support decisions, not silently replace them. Human oversight must be meaningful, which means humans need the authority, training, and time to challenge system outputs. A nominal human-in-the-loop is not enough if the human cannot realistically override the system.
Digital governance also has a trust dimension. Affected populations may experience data collection as extraction or surveillance if purpose, use, sharing, retention, and grievance routes are unclear. The Global Digital Compact’s human-centered and rights-oriented language must be translated into operational controls. Strategic risk management is where that translation should happen.
5.8 Efficiency Must Not Become Hidden Risk Transfer
Efficiency matters. Resources are limited and needs are high. The UN system has a duty to reduce duplication, improve procurement, share services where sensible, simplify processes, and direct more resources toward mandate delivery. But efficiency has to be tested for risk transfer.
A cut that removes waste strengthens the system. A cut that removes redundancy may weaken crisis readiness. A shared service may reduce cost and increase consistency, or it may create dependency and a single point of failure. A streamlined approval process may reduce delay, or it may weaken safeguards if poorly designed. A reduction in monitoring cost may look efficient until a safeguarding failure or fraud risk emerges. The question is not whether efficiency is desirable. It is what kind of capacity is being removed.
This is particularly important under funding pressure. Prevention, training, evaluation, partner support, cybersecurity, knowledge management, and duty-of-care arrangements often look easier to cut than frontline delivery. Yet these functions protect the credibility and safety of frontline delivery. Strategic risk leadership should distinguish administrative burden from protective capacity. The first should be reduced. The second should be preserved.
Efficiency should therefore be risk-adjusted. Before major savings are adopted, leaders should ask: what risk does this create, who will absorb it, what control replaces the removed capacity, how will we know if the saving damages delivery, and what trigger would reverse the change? This is not resistance to reform. It is disciplined reform.
Chapter 6: Applied Diagnostic Tools
The models in this chapter are designed for use, not decoration. Their value lies in helping leadership teams ask better questions and record clearer decisions. A UN audience will rightly distrust tools that hide assumptions. The formulas here are intentionally simple. They can be adapted, weighted differently, or expanded as evidence improves.
The strongest use of the tools is not a one-time score. It is repeated review. A country team might use SRLI quarterly, DLD for selected decision processes, RARD during results reporting, PTAS before scaling partnerships, and scenario stress tests before major programme expansion. Over time, the tools create a management memory: which risks were known, what changed, what did not change, and why.
6.1 Using the Strategic Risk Leadership Index
SRLI should be conducted in a structured session with cross-functional participation. The group should include programme leadership, operations, finance, procurement, risk, monitoring and evaluation, safeguarding, data protection, security, and partner representation where appropriate. Each variable should be scored with evidence. Where evidence is weak, the score should be marked as uncertain rather than inflated.
The most valuable moment is disagreement. If headquarters scores resource mobility high and a field office scores it low, the difference reveals a practical issue. If a local partner scores role clarity low while the UN entity scores it high, the partnership design needs review. If safeguarding staff score controls lower than programme managers do, the organization should listen carefully. The index should make these differences visible.
A recommended scoring protocol has four steps: collect evidence before the session, score each variable individually, compare the scores and discuss the gaps, and record two or three decisions. The process should not end with a chart. It should end with action: clarify authority, adjust funding, strengthen partner support, revise data controls, or escalate a risk to a senior forum.
6.2 Interpreting Risk-Adjusted Results
The RARD model should be applied when a programme claims success under risk. It does not require a complex mathematical system at the beginning. A light version can use qualitative ratings: strong, adequate, weak, or critical. The point is to attach results to interpretation.
For example, a programme may report that it reached 100,000 people with assistance. RARD asks: was the assistance delivered to standard? Were marginalized groups reached? Can the result persist? What residual risks remain? Was there any harm, exclusion, complaint pattern, or safeguarding concern? If quality is low, equity is weak, sustainability is fragile, and residual risk is high, the headline number must be interpreted differently.
RARD also helps donors. Donors often demand evidence of scale and value for money. Risk-adjusted reporting shows value more honestly. It can explain why reaching fewer people in a high-risk area may be more strategically important than reaching more people in an easier area. It can also show why a programme should slow scale until safeguards or data controls are adequate.
6.3 Using the Decision-Lag Diagnostic
DLD should be applied to selected high-risk processes: emergency response, procurement under crisis conditions, safeguarding escalation, data incident response, partner agreement approval, funding reallocation, and access negotiation. The team should map the most recent case and record elapsed time across each stage. Then it should ask which delay was necessary and which was avoidable.
The corrective action must fit the delay. If signal recognition is slow, strengthen field intelligence and partner feedback. If analysis is slow, improve data integration and risk methodology. If approval is slow, clarify authority. If resource release is slow, negotiate flexible funding or contingency budgets. If partner alignment is slow, use pre-agreed roles or framework agreements. If feedback review is slow, create a management response tracker.
The diagnostic is also useful for governing bodies because it shifts oversight from general concern to concrete process. Instead of asking why the organization was slow, oversight can ask where the decision cycle slowed and what control will change.
6.4 Using the Partner Trust and Accountability Score
PTAS should be used before partnerships are scaled and during periodic partner review. It should be completed by both the UN entity and the partner. Differences in scores are important. A UN office may believe funding reliability is acceptable because disbursements comply with internal timelines; a local partner may experience the same timing as operationally damaging because it must pay staff or suppliers before reimbursement. Both perspectives are evidence.
The score should also be linked to risk allocation. A partnership that assigns high delivery risk to a local actor should provide corresponding support: overhead, security arrangements, training, data systems, safeguarding capacity, insurance or equivalent risk cover, and dispute routes. If the support is absent, the risk allocation is not credible.
PTAS can prevent localization from becoming rhetoric. A locally led response is not achieved by placing more obligations on local organizations. It is achieved by sharing authority, resources, information, and accountability in ways that make local leadership sustainable.
6.5 Scenario Stress-Test Scoring
A simple scenario score may be calculated as:
Scenario Stress Score = (Exposure × Probability × Consequence × Recovery Time) − Preparedness Capacity
Exposure measures the scale of the affected programme or population. Probability estimates how plausible the shock is within the planning period. Consequence measures harm to people, mandate delivery, finance, safety, trust, and legal obligations. Recovery time estimates how long it would take to restore minimum function. Preparedness capacity subtracts the strength of existing controls, contingency arrangements, flexible funding, trained staff, partner agreements, and communication plans.
The score should not create false precision. Its purpose is to force explicit discussion of assumptions. If a programme depends on one donor, one access route, one data platform, one implementing partner, or one political approval chain, the stress test will reveal fragility. Leadership can then redesign before scale locks in the weakness.
Table 4. Decision-lag stages and corrective actions
| Stage | Diagnostic question | Common cause of delay | Corrective action |
| Signal recognition | How quickly did the organization notice the risk? | Weak field intelligence or partner feedback | Strengthen early warning, community feedback, and partner escalation |
| Risk analysis | How quickly was the signal interpreted? | Fragmented data or unclear method | Create rapid risk notes and integrated data review |
| Approval | Who had authority to act? | Overcentralization or unclear delegation | Clarify decision rights and escalation thresholds |
| Resource release | How quickly did funds, staff, or supplies move? | Rigid budget or donor restrictions | Build flexible funding, contingency lines, donor pre-approval |
| Partner alignment | Were partners ready to adjust? | Unclear roles or contract rigidity | Use framework agreements and role maps |
| Field start | When did action begin? | Procurement, staffing, security, or logistics barriers | Pre-position supplies, rosters, and security protocols |
| Feedback review | Did the system learn from the response? | No owner for management response | Track actions, deadlines, and evidence of completion |
Chapter 7: Implementation Blueprint for UN-Aligned Organizations
An organization seeking to work credibly with the United Nations should not approach UN alignment as a branding exercise. It should be able to demonstrate that its governance, safeguards, data practices, financial controls, partner relationships, and learning systems are strong enough for complex mandate work. The UN system is increasingly attentive to risk-informed programming, responsible digital cooperation, results credibility, localization, and resilience. A partner that cannot document its own controls becomes a risk multiplier, no matter how attractive its proposal appears.
This chapter translates the diagnostic framework into a practical blueprint for UN-aligned organizations, country teams, and partner consortia.
7.1 Governance Readiness Review
Before seeking serious UN partnership, an organization should conduct a governance readiness review. The review should examine board oversight, executive accountability, financial controls, segregation of duties, procurement, anti-fraud practice, safeguarding, data governance, complaint handling, staff capacity, duty of care, monitoring and evaluation, and community accountability. The output should be an evidence file, not a promotional brochure.
The review should identify red flags. These include unclear authority, no documented safeguarding pathway, no incident reporting process, weak audit trail, informal procurement, no data retention rule, inadequate partner due diligence, missing conflict-of-interest controls, and dependence on one individual for institutional memory. These weaknesses are common in growing organizations. They become dangerous when hidden. A partner that acknowledges weakness and has a credible repair plan is more trustworthy than one that claims maturity without evidence.
Proportionality matters. A small local organization should not be expected to imitate the administrative infrastructure of a large UN agency. But proportionality is not an excuse for unsafe practice. The standard is whether the organization understands the risks attached to its role and has controls appropriate to its size, mandate, and operating context.
7.2 Mandate Translation
UN-aligned organizations should be able to state precisely which UN priority they support, which population they serve, which policy or operational need they address, and which risks they recognize. Generic references to the Sustainable Development Goals are not enough. A credible proposal should connect to a specific need: food security, health preparedness, child protection, displacement response, climate adaptation, governance support, digital inclusion, peacebuilding, gender equality, social protection, or local resilience.
Mandate translation prevents opportunistic alignment. It also helps reviewers test whether the organization understands the political and ethical conditions of the work. A digital education proposal for displaced children, for example, must address connectivity, language, disability inclusion, child safeguarding, data protection, teacher support, psychosocial needs, host-community relations, and sustainability. A proposal that speaks only about technology is not mandate-ready.
The strongest proposals state the trade-offs. They explain what the organization will do, what it will not do, what assumptions must hold, what risks remain, and what decision points would trigger redesign. This candor is a mark of maturity, not weakness.
7.3 Country-Level Application
Strategic risk management becomes most useful at country level because that is where global priorities meet political economy, local institutions, security conditions, climate exposure, social norms, market realities, and community trust. A global strategy may identify the right themes, but a country team must decide which risks are immediate, which are structural, and which actors can realistically move them.
A country-level risk review should involve programme teams, operations, security, finance, procurement, data protection, safeguarding, monitoring and evaluation, local partners, government counterparts where appropriate, and affected community feedback. It should not be a headquarters exercise performed at distance. The most important risk signals often sit close to implementation.
One practical tool is the ninety-day risk action memo. Every quarter, the leadership team records the three most important risk signals, the decision taken, the owner, the resource implication, the safeguard implication, and the next review date. The memo should be short. Its value is that it reduces the distance between risk awareness and decision. It also creates institutional memory when staff rotate.
7.4 Partner Risk Allocation
Partnership agreements should include a risk allocation section. This section should identify who carries delivery risk, security risk, safeguarding risk, fiduciary risk, data risk, reputational risk, and cash-flow risk. It should also identify what support accompanies each responsibility. If a local partner is responsible for sensitive data collection, it needs data protection training, secure systems, and clear sharing rules. If it is responsible for safeguarding referrals, it needs survivor-centered protocols and safe complaint pathways. If it is expected to deliver in insecure areas, duty-of-care arrangements cannot be vague.
Donors and UN entities should examine payment timing and overhead honestly. Late reimbursement can push smaller partners into debt or force them to delay staff salaries. Overhead restrictions can prevent partners from building the systems donors later demand. Excessive reporting can consume the very capacity needed for delivery. Risk-informed partnership is not a demand for lower standards. It is a demand that standards be resourced.
A partner risk meeting should occur before scale, not after problems appear. The meeting should ask what failure would look like, who would see it first, how it would be reported, and how the partnership would respond. This is a better use of time than assuming goodwill will solve structural strain.
7.5 Data and Digital Assurance
Every UN-facing organization that handles personal or sensitive data should maintain a data and digital assurance file. The file should state the purpose of data collection, the legal or ethical basis, the minimum data required, consent or alternative justification, retention period, sharing rules, security controls, breach response, human oversight, and grievance route. Where AI or automated decision support is used, the file should include bias review, explainability limits, override authority, and monitoring.
Data protection should be connected to programme design. It is not enough for an organization to have a policy. The question is how the policy affects field practice. Are enumerators trained? Are devices secure? Are paper records protected? Are vulnerable people told how data will be used? Can they correct errors? Who can access the database? What happens if a partner leaves the consortium? What happens if government requests conflict with protection concerns?
Digital assurance is also about inclusion. A tool that assumes smartphones, literacy, stable connectivity, official identity documents, or language fluency may exclude precisely those whom the programme is meant to serve. Accessibility, offline options, human support, and alternative pathways are not secondary design choices. They are risk controls.
7.6 Evaluation as a Management Trigger
Evaluation should trigger management action, not only institutional reflection. Each recommendation should have an owner, deadline, resource implication, and verification method. If leadership rejects a recommendation, the reason should be recorded. If action requires donor flexibility, the donor should be engaged. If action requires partner capacity, support should be built into the next workplan.
A management response without follow-up is a polite ritual. The organization can say it has learned, but learning remains unproven. A stronger approach tracks recommendation status over time: accepted, partially accepted, rejected, in progress, completed, verified, or superseded. The tracker should be reviewed by leadership, not left as an evaluation-office file.
Learning should also be shared with partners and affected communities where appropriate. If people provided feedback or suffered from a programme weakness, they should not disappear from the learning process. Accountability includes explaining what changed.
Chapter 8: Scenario Stress Tests
Scenario stress testing helps leaders examine whether a plan can survive plausible disruption. It is not prediction. It is a disciplined way to expose fragile assumptions. Many strategies assume stable access, donor continuity, partner capacity, data availability, staff safety, government cooperation, and community acceptance. Any one of those assumptions can fail. In compound risk settings, several may fail together.
The following stress tests can be used by UN entities, country teams, partner organizations, donors, and academic training programmes.
8.1 Funding Contraction
The team assumes a thirty percent funding reduction over six months. It asks which outputs stop, which staff roles become critical, which partners face cash-flow risk, whether safeguarding or monitoring would be weakened, which affected groups lose support first, and how the organization would communicate prioritization. This scenario is essential because funding contraction rarely affects all activities equally. It exposes the real hierarchy of priorities.
The leadership question is not simply what can be cut. It is what must be protected because cutting it would create disproportionate harm. Monitoring, safeguarding, security, and partner support may appear indirect, but removing them can make frontline delivery unsafe or unaccountable. A risk-informed budget cut protects the functions that protect people.
The scenario should produce pre-agreed prioritization rules. Waiting until money is gone invites hurried and opaque decisions. Donors should be involved where restrictions prevent adaptive action. A funding contraction plan should identify minimum service packages, decision thresholds, and communication duties.
8.2 Access Deterioration
The team assumes that conflict, bureaucracy, insecurity, disaster, or political tension reduces access to key locations. It asks whether remote management is safe, whether local partners can carry delivery, whether data quality can be maintained, how affected communities will communicate needs, and whether staff and partner security protocols are adequate.
This scenario tests whether localization is supported or merely assumed. If local partners become the only route to delivery, they need resources, security guidance, communication channels, and authority to adapt. Remote management can protect international staff while increasing local partner exposure. Risk leadership must not allow that transfer to remain invisible.
Access deterioration also tests data integrity. When direct monitoring becomes difficult, organizations may rely on partner reports, third-party monitors, remote sensing, call centers, or community feedback. Each method has limits. The stress test should identify how triangulation will occur and what uncertainty will be reported.
8.3 Data Failure
The team assumes that a data platform becomes unreliable, unavailable, compromised, biased, or ethically contested. It asks what decisions depend on the platform, what manual or alternative procedures exist, how personal data will be protected, whether affected people can challenge errors, and who has authority to suspend the tool.
Data failure is increasingly strategic because digital systems are becoming central to targeting, registration, payments, supply planning, monitoring, and reporting. A platform failure can become a protection failure, cash failure, trust failure, or public communication failure. The stress test should therefore include technical, legal, ethical, and operational staff.
The most important question is whether human judgment can still function. If staff cannot explain or override the system, the organization has created dependency. Digital modernization should increase capability, not reduce institutional judgment.
8.4 Legitimacy Shock
The team assumes that public trust declines because of misinformation, a safeguarding incident, a contested partnership, a data breach, poor communication, corruption allegation, or political backlash. It asks who communicates, what evidence is available, how complaint channels work, whether partners are aligned, and how the organization will act without becoming defensive.
Legitimacy shocks often begin in perception, but they can quickly become operational. Communities may refuse assistance, staff may face hostility, access may narrow, donors may suspend funds, and partners may distance themselves. The response must therefore be factual, transparent, and protective. Hiding problems usually deepens the shock.
A legitimacy stress test should include pre-approved communication principles: tell the truth quickly, protect confidentiality, acknowledge uncertainty, state what is being done, avoid blaming affected people or partners, and provide routes for complaint and correction. Trust is not preserved by image management. It is preserved by credible action.
8.5 Combined Shock
The most realistic test is combined shock. The team assumes that funding falls, access deteriorates, data become unreliable, and public trust weakens in the same quarter. This is not pessimism. It reflects the way compound crises behave. One shock often triggers another. Funding cuts may reduce monitoring. Reduced monitoring may weaken data. Weak data may create targeting errors. Targeting errors may damage trust. Damaged trust may reduce access.
A combined-shock exercise should identify minimum viable mandate delivery. What must continue? Which populations are highest priority? Which safeguards cannot be suspended? Which decisions can be delegated? Which partnerships must be reinforced? Which communications are required? The exercise should end with a short action plan and named owners.
This is also a useful training tool for NYCAR classes. Students can be assigned roles – country director, risk officer, local partner, donor, safeguarding adviser, data protection officer, community representative – and asked to negotiate decisions under constraint. The exercise teaches that risk leadership is not abstract. It is the art of making defensible choices when every option has a cost.
Chapter 9: Ethics, Safeguards, and Political Realism
Strategic risk management in the UN system cannot be ethically neutral. It concerns people whose lives, rights, safety, dignity, and future opportunities are affected by institutional choices. A risk framework that protects the organization while ignoring those people has failed at the level of mandate.
At the same time, ethics without political realism can become performative. UN entities operate through member states, governing bodies, donors, host governments, legal constraints, security environments, and public scrutiny. A serious framework must be morally clear and politically literate. It must recognize constraints without letting constraints become excuses for avoidable harm.
9.1 Safeguarding as Strategic Risk
Safeguarding is often treated as a specialized compliance area. It should also be understood as strategic risk because abuse, exploitation, harassment, retaliation, and unsafe complaint systems can destroy trust, harm people, damage access, and invalidate results. A programme that delivers outputs while exposing people to abuse has not succeeded. It has failed at the most basic level of responsibility.
Safeguarding must be resourced. Training, complaint pathways, survivor-centered response, partner support, investigation capacity, monitoring, and leadership accountability require time and money. Under funding pressure, these functions may appear indirect. They are not. They are protective infrastructure.
Safeguarding also has a partner dimension. Local partners may be required to meet standards without adequate support. This creates both compliance risk and ethical risk. A UN-facing organization should not impose standards it is unwilling to help partners implement. The right approach is firm expectations plus practical capacity support.
9.2 Human Rights and Data Risk
Data governance is a rights issue when information concerns refugees, displaced people, children, survivors of violence, people living with disease, political dissidents, undocumented migrants, or communities in conflict areas. Data can help target assistance and protect people. It can also expose them. The same dataset that improves delivery may become dangerous if shared with the wrong actor, breached, retained too long, or used for a purpose people did not understand.
A rights-sensitive data practice begins with purpose. Why is the data needed? What is the minimum necessary? Who will access it? How long will it be kept? Can people refuse without losing essential assistance? Can they correct errors? What happens if authorities request access? What safeguards apply if the data concern children or protection risks? These are not technical afterthoughts. They are programme design questions.
AI and automated decision support require even stronger caution. A model may produce a score, but affected people need a route to contest decisions. Human oversight must be meaningful. Sensitive decisions affecting access to assistance, protection referrals, or eligibility should not be reduced to opaque automation. The human rights standard is not satisfied by speed alone.
9.3 Political Realism
Political realism means recognizing that risk decisions occur in contested environments. Member states may disagree. Host governments may resist scrutiny. Donors may earmark funds. Communities may distrust institutions. Armed actors may manipulate access. Public narratives may be distorted. The UN system must navigate these realities without surrendering mandate integrity.
Risk leadership therefore includes diplomatic judgment. Not every risk can be announced publicly in the same way. Not every trade-off can be solved by technical design. Some choices require negotiation, advocacy, quiet escalation, coalition-building, or phased action. But political complexity should not become a cover for silence. Leaders should record what is known, what is constrained, which options were considered, and why a decision was made.
This is especially important when resources are insufficient. Scarcity can force tragic choices. Ethical leadership does not pretend otherwise. It makes prioritization criteria explicit, protects the most vulnerable where possible, explains trade-offs to donors and affected communities, and records residual harm honestly. The absence of resources may explain a failure to deliver everything. It does not justify dishonest reporting.
9.4 Trust as a Strategic Asset
Trust affects access, safety, participation, reporting, fundraising, and legitimacy. It should therefore be measured and managed as a strategic asset. Trust is built through delivery, honesty, safeguards, responsiveness, and respect. It is weakened by inflated claims, opaque decisions, unaddressed complaints, extractive data practices, late payments to partners, and defensive communication.
Organizations should measure trust through multiple signals: community feedback, complaint data, partner surveys, staff morale, donor confidence, media analysis, access negotiations, and programme participation. None of these signals is perfect. Together, they can show whether accountability is visible.
Trust is not protected by hiding problems. It is protected by facing them. Affected people and partners do not expect perfection. They are more likely to trust institutions that acknowledge failure, correct it, and explain what changed. Strategic risk management therefore turns trust from a public relations concern into a performance condition.
Chapter 10: Sector-Specific Strategic Risk Files
Sector files translate the general framework into applied areas. Each file identifies the risk pattern, the leadership question, and the evidence that should be requested. The files are not exhaustive. They are meant to help UN-facing organizations build sharper risk notes for different mandate areas.
10.1 Food Security and Hunger Risk
Food security risk is immediate because consequences are bodily and time-sensitive. Delays, access restrictions, supply failure, funding cuts, inflation, market disruption, and targeting errors can quickly become malnutrition, hunger, displacement, or social tension. The leadership question is whether the organization can protect life-saving assistance while making prioritization transparent and accountable.
Evidence should include food security analysis, market monitoring, supply-route risk, pipeline status, partner capacity, protection analysis, targeting criteria, community feedback, and complaint data. Risk-adjusted results should report not only people reached but adequacy, timeliness, inclusion, and residual unmet need. Under funding contraction, leaders should state what ration reductions or prioritization decisions mean for affected people.
Innovation in food security should be judged by field usefulness. Digital payments, satellite analytics, AI-assisted vulnerability analysis, and supply-chain tools can help, but only if data quality, privacy, inclusion, and explainability are protected. The test is whether the tool improves decisions for hungry people, not whether it impresses institutional audiences.
10.2 Refugee Protection and Displacement Risk
Displacement risk is political, legal, social, and operational. Refugees, asylum seekers, internally displaced persons, stateless people, and host communities face risks that cannot be solved by assistance alone. Documentation, legal status, protection from refoulement, family unity, gender-based violence prevention, shelter, education, livelihoods, health, and durable solutions all interact.
The leadership question is whether results reporting remains attached to protection meaning. How many people were registered matters. Whether registration protected confidentiality and improved access to rights also matters. How many shelters were provided matters. Whether women, children, older persons, persons with disabilities, and marginalized groups were safe also matters.
Evidence should include protection monitoring, legal access data, community feedback, complaint systems, referral pathways, confidentiality controls, data-sharing agreements, host-community analysis, and durable-solution prospects. Strategic risk management should resist any performance narrative that counts activity while ignoring legal and protection conditions.
10.3 Development Governance and Institutional Risk
Development governance risk often appears slowly. A programme may achieve outputs while leaving institutions unable to sustain them. Climate shock, corruption, weak public finance, political turnover, conflict, or debt distress can undermine gains after the project closes. The leadership question is whether development investments are risk-proofed against foreseeable shocks.
Evidence should include political economy analysis, institutional capacity assessment, fiscal sustainability, climate risk screening, procurement integrity, public finance implications, stakeholder ownership, and maintenance plans. Development results should be judged partly by whether local systems can continue the work.
Risk-informed development also requires humility about external support. International assistance can strengthen national capacity, but it can also create dependency or parallel systems. The test is whether local institutions, civil society, and communities gain capability, authority, and resources that survive beyond the project cycle.
10.4 Child-Focused Systems and Intergenerational Risk
Child-focused risk is cumulative. Harm that occurs early can shape education, health, protection, income, and social participation for a lifetime. Conflict, displacement, climate shock, poverty, gender inequality, disability exclusion, violence, and digital harm often interact. The leadership question is whether programmes protect the children most likely to be missed by scale.
Evidence should include disaggregated data, child safeguarding, disability inclusion, gender analysis, education continuity, nutrition status, WASH access, social protection coverage, community feedback, and safe child participation. Results should be adjusted for equity. A large programme that misses excluded children has limited strategic value.
Intergenerational risk also requires long-term thinking. Cutting education in emergencies, underfunding adolescent girls, neglecting child protection, or ignoring mental health may appear to save resources in the short term. The future cost is high. Strategic risk management should make that cost visible.
10.5 Public Health Preparedness and Trust Risk
Public health preparedness risk is often politically invisible until the emergency arrives. Surveillance, laboratories, workforce training, community engagement, emergency coordination, supply readiness, and financing mechanisms are easier to neglect than emergency response. The leadership question is whether preparedness is treated as a measurable result.
Evidence should include readiness assessments, surveillance coverage, laboratory capacity, workforce training, supply plans, emergency operations arrangements, risk communication capacity, community trust data, and flexible funding. Preparedness reporting should show not only activities completed but response capability improved.
Trust is central. Communities must believe guidance, report symptoms, accept services, and understand uncertainty. Misinformation, attacks on health care, politicized guidance, and poor communication can weaken response. Public health risk leadership therefore includes social listening, local partnership, transparent communication, and protection of health workers.
10.6 Digital Cooperation and Information Integrity
Digital cooperation risk cuts across sectors. Data systems, AI tools, digital public infrastructure, biometric registration, cash platforms, remote monitoring, and communication systems can improve performance. They can also create exclusion, surveillance risk, cyber exposure, bias, and misinformation. The leadership question is whether digital tools are governed as rights-sensitive operations.
Evidence should include data protection impact assessment, cybersecurity review, accessibility testing, algorithmic risk analysis, human oversight rules, grievance mechanisms, vendor due diligence, interoperability plans, and shutdown conditions. Digital results should report who was excluded, what errors occurred, and how complaints were resolved.
Information integrity is now a strategic risk. Disinformation can damage vaccination, humanitarian access, trust in refugee services, election support, climate action, and peacebuilding. Institutions must monitor information environments without manipulating communities. The ethical line is clear: risk communication should inform, listen, and correct; it should not deceive.
10.7 Climate and Future Generations Risk
Climate risk is both immediate and intergenerational. Droughts, floods, heat, storms, sea-level rise, crop loss, water stress, and displacement affect health, food, education, protection, and public finance. The leadership question is whether programmes are designed for climate conditions that are already foreseeable.
Evidence should include climate risk screening, adaptation analysis, early warning, local knowledge, environmental safeguards, contingency plans, and financing for resilience. Climate risk should not be handled only by environment teams. It belongs in education planning, health systems, food security, social protection, procurement, infrastructure, and displacement response.
Future generations language requires more than moral appeal. It requires present decisions that reduce long-term exposure. When budgets cut preparedness, adaptation, education, health prevention, or child protection, they may be transferring risk to people who cannot vote in current budget cycles. Strategic risk management gives leaders a vocabulary for naming that transfer.
Chapter 11: Recommendations
The recommendations below are designed for UN entities, country teams, donors, governing bodies, partner organizations, and UN-facing institutions. They should be adapted to mandate, legal status, context, and scale. They are not a universal checklist. They are a disciplined starting point.
11.1 Place Risk Review Inside Strategic Decision Forums
Risk review should not sit only in audit or compliance meetings. It belongs in strategic planning, programme approval, budget review, partner selection, procurement, safeguarding escalation, data governance, emergency response, and evaluation follow-up. Every major decision should include a short risk intelligence note identifying the top risks, recent field signals, proposed treatment, owner, residual exposure, and decision required.
This recommendation matters because risk only changes performance when it changes choices. A long risk annex buried in a report is less useful than a one-page risk note presented at the moment of decision. Leaders need concise, evidence-backed risk intelligence at the table where authority is exercised.
11.2 Link Foresight to Budget Flexibility
Foresight should trigger resource options. If scenarios identify likely funding, conflict, climate, health, digital, or legitimacy shocks, the organization should identify flexible funding, contingency procurement, surge capacity, partner agreements, or communication plans. A scenario without a resource option is not yet operational.
Donors and governing bodies should support adaptive funding with accountability. Flexibility does not mean weaker reporting. It means reporting on adaptive decisions, documented trade-offs, and changed conditions rather than forcing programmes to pretend that the original plan still fits.
11.3 Build Risk-Adjusted Results Reporting
Results reports should include risk-adjusted interpretation. Programmes should report what was achieved, whether quality standards held, which groups were reached or missed, what risk was reduced, what residual exposure remains, what complaints or harm concerns arose, and what changed in the next phase.
This will make reporting more honest and more useful. It will also protect organizations from inflated success claims that later collapse under scrutiny. Donors should welcome this approach because it provides a more accurate view of value.
11.4 Shorten Decision Lag Without Weakening Safeguards
Organizations should measure decision lag in selected high-risk processes. Emergency response, safeguarding escalation, procurement, funding reallocation, data incident response, partner agreement approval, and access negotiation are good starting points. The goal is not speed at any cost. The goal is timely, proportionate authority.
Safeguards should be built into rapid action. Prepared organizations can move quickly because roles, templates, escalation routes, partner vetting, legal guidance, and contingency funds are pre-agreed. Slow processes are sometimes defended as careful, but weak preparedness can masquerade as care.
11.5 Protect Local Partners From Hidden Risk Transfer
Localization and partnership reform should include honest risk allocation. UN entities and donors should examine payment timing, overhead, reporting burden, security support, safeguarding capacity, data systems, training, and dispute resolution. Local partners should not be expected to carry delivery, security, safeguarding, and cash-flow risk without authority and support.
The PTAS model can be used as a pre-scale review. If trust conditions are weak, the partnership should be strengthened before larger responsibilities are assigned. Strategy should not depend on partner heroism.
11.6 Govern Data, Digital, and AI as Rights-Sensitive Operations
Digital projects in UN contexts should be reviewed for purpose, privacy, security, inclusion, explainability, human oversight, bias, grievance routes, and shutdown conditions. Sensitive data and AI systems should not be scaled until governance is ready. A tool that cannot be explained to affected people or staff is not ready for high-risk deployment.
This recommendation is especially important after the Global Digital Compact. The UN system can lead by showing that digital modernization and rights protection can move together. Trust will be the measure of success.
11.7 Use Evaluation as a Management Trigger
Evaluation recommendations should be connected to owners, deadlines, resources, and follow-up evidence. Leadership should review implementation status. Rejected recommendations should include reasons. Accepted recommendations should show what changed.
This transforms evaluation from a retrospective product into a management control. It also helps institutions retain learning despite staff turnover and emergency pressure.
11.8 Make Trust Measurable
Trust should be measured through community feedback, complaint systems, partner surveys, donor confidence, staff signals, access conditions, and public communication evidence. Trust is not public relations. It is an operating condition. Affected people should know how to complain, partners should be able to challenge unrealistic plans, and public claims should be supported by evidence.
Trust is protected when institutions tell the truth, correct failure, and show that feedback changes action.
Table 5. Recommendations and evidence for oversight
| Recommendation | Reason | Evidence to request |
| Place risk in strategic forums | Risk matters when it changes choices. | Decision notes, owners, residual exposure, meeting records |
| Link foresight to budget flexibility | Future risks need present options. | Scenario triggers, contingency funds, donor flexibility |
| Use risk-adjusted results | Outputs can hide exclusion, harm, and fragility. | Quality, equity, sustainability, residual risk, harm review |
| Measure decision lag | Late decisions can perform like wrong decisions. | Elapsed days by stage, corrective actions |
| Protect local partners | Partnership can transfer risk downward. | Payment timing, overhead, role clarity, safeguarding support |
| Govern data and AI | Digital systems can create rights and trust risks. | Privacy review, cybersecurity, human oversight, grievance route |
| Use evaluation as trigger | Learning matters only when management changes. | Management response tracker, verification evidence |
| Measure trust | Trust affects access, reporting, safety, and legitimacy. | Feedback data, complaint analysis, partner surveys, communication evidence |
Chapter 12: Limitations and Research Agenda
The research has clear limitations. It is based on public documentary evidence and does not claim access to confidential UN decision-making, internal risk registers, internal audit files beyond public documents, country-level dashboards, or staff interviews. It therefore cannot determine whether any specific entity consistently applies the practices described. It can analyze formal intent, public management logic, and visible evidence of institutional priorities, but not the full internal sequence of decisions.
The diagnostic models are conceptual. They have not been statistically validated. Their weights are reasoned rather than empirically derived. In practice, weights should be adapted to mandate and context. A humanitarian logistics operation may weight resource mobility more heavily. A protection agency may weight safeguards and trust more heavily. A health emergency function may weight preparedness, surveillance, and communication. A development governance programme may weight sustainability and national systems.
Scoring also depends on honesty. Organizations may overrate themselves, especially when scores are linked to external reputation. The models should therefore be used for internal learning before external reporting. When used for oversight, scores should be supported by evidence and open to partner and field challenge. Without contested evidence, the models could become another performance ritual.
Context also matters. A low SRLI score may indicate weak leadership, but it may also indicate an extreme operating environment, donor inflexibility, insecurity, or political constraints. The models should not punish teams for naming hard realities. In fact, an honest low score may be more useful than an inflated high score. The purpose is improvement, not public ranking.
Future research should test the models through case studies at country level. Researchers could apply SRLI, DLD, RARD, and PTAS to selected programmes across humanitarian, development, protection, and health contexts. They could compare leadership perceptions with partner and community perceptions. They could examine whether decision-lag reduction improves results quality. They could test whether risk-adjusted reporting changes donor dialogue. They could explore how digital governance affects trust in different contexts.
A second research agenda concerns funding flexibility. Many strategic risk failures are tied to resource rigidity. Future studies should examine which donor instruments allow adaptive management without weakening accountability. This could include pooled funds, crisis modifiers, contingency lines, adaptive workplans, and results reporting that accepts justified change.
A third agenda concerns local partners. Researchers should examine how risk is allocated in partnership agreements and whether localization reforms are accompanied by overhead, duty-of-care support, safeguarding capacity, data systems, and dispute mechanisms. Without this work, localization risks becoming an attractive term that hides unequal exposure.
A fourth agenda concerns AI and data in UN-facing operations. As AI tools become more common, researchers should study explainability, human oversight, bias, exclusion, grievance routes, procurement standards, and accountability when automated systems influence assistance, protection, or public services. This research must be interdisciplinary, combining technology governance with human rights, humanitarian ethics, and field operations.
A final agenda concerns institutional culture. Risk tools do not work if leaders punish bad news. Future research should study psychological safety, escalation behavior, leadership incentives, and the relationship between organizational culture and decision lag. The strongest risk framework will fail if staff and partners do not believe that truth can travel upward safely.
Chapter 13: Conclusion and Executive Note
Strategic risk management for United Nations system performance is leadership under constraint. It is the discipline of making mandate delivery more dependable when the operating environment is unstable and when failure carries human consequences. The UN system already has substantial strategy language, reform agendas, and risk tools. The next test is whether these instruments change decisions quickly, honestly, and ethically enough to protect results.
This research has argued that risk is not a compliance annex. It is a leadership signal, a results condition, a partner issue, a digital governance challenge, a future generations concern, and a trust matter. UN 2.0 and the Pact for the Future provide a strong reform platform, but their value will depend on translation into operating choices. Data, digital tools, innovation, foresight, and behavioural science will improve multilateral performance only if they are linked to safeguards, field usability, budget authority, partner support, and evidence learning.
The case readings show that strategic risk differs by mandate. WFP is tested by hunger, supply chains, prioritization, funding pressure, and innovation. UNHCR is tested by displacement, protection, data responsibility, results integrity, and evaluation follow-up. UNDP is tested by risk-informed development, governance, climate exposure, and national systems. UNICEF is tested by child-centered equity, systems resilience, and intergenerational harm. WHO is tested by preparedness, health emergencies, trust, and flexible financing. System-wide reform is tested by whether broad agendas become daily management decisions.
The diagnostic tools introduced here are intentionally practical. The Strategic Risk Leadership Index examines whether leadership conditions exist. The Risk-Adjusted Results Delivery model protects against output reporting that hides risk. The Decision-Lag Diagnostic shows where risk intelligence slows before action. The Partner Trust and Accountability Score treats partnership quality as a delivery control. Scenario stress testing forces strategies to confront plausible disruption. None of these tools replaces judgment. They discipline judgment.
For organizations seeking to be attractive to the UN system, the lesson is clear. They should not approach the UN with fashionable language alone. They should demonstrate risk-informed planning, credible safeguards, responsible data governance, partner discipline, financial control, evaluation follow-up, and the ability to adapt without losing accountability. They should be able to show how they protect people, manage resources, learn under pressure, and make trade-offs visible.
The final professional judgment is direct. Multilateral strategy will be credible only when it becomes operationally answerable. Leaders must be able to say what risk was seen, who acted, what changed, which trade-off was accepted, what harm was prevented, which result survived, and what was learned. In a world of compound risk, that discipline is not administrative refinement. It is part of the moral and practical work of international cooperation.
Executive Note for UN-Oriented Review
This research paper is suitable for an advanced NYCAR class on strategic risk management, institutional leadership, public administration, and UN-facing policy practice. It gives students and practitioners a framework for examining how multilateral organizations move from risk awareness to decision accountability. Its value lies in the combination of ethical seriousness and management discipline.
The research should be read as an applied model-building study, not as an investigative audit. Its strongest classroom use is as a diagnostic exercise. Students can select a UN programme, country strategy, or partner proposal and apply SRLI, RARD, DLD, PTAS, and scenario stress testing. They should be asked to identify evidence, challenge assumptions, and explain trade-offs. That will teach the central lesson: risk leadership is not the act of listing dangers. It is the act of making defensible decisions when mandate, resources, uncertainty, and human stakes collide.
References
Joint Inspection Unit. (2017). Results-based management in the United Nations system: Description of a high-impact model for managing for achieving results (JIU/NOTE/2017/1). United Nations.
Joint Inspection Unit. (2020). Enterprise risk management: Approaches and uses in United Nations system organizations (JIU/REP/2020/5). United Nations.
United Nations. (2023). UN 2.0: A United Nations ready for the future. United Nations.
United Nations. (2024). Pact for the Future, Global Digital Compact and Declaration on Future Generations (A/RES/79/1). United Nations.
United Nations Development Programme. (2021). Risk-informed development: A strategy tool for integrating disaster risk reduction and climate change adaptation into development. UNDP.
United Nations Children’s Fund. (2021). UNICEF Strategic Plan 2022-2025. UNICEF.
United Nations Children’s Fund. (2025). UNICEF Strategic Plan 2026-2029 (E/ICEF/2025/29). UNICEF Executive Board.
United Nations High Commissioner for Refugees. (2024). Strategy for evaluation in UNHCR 2024-2027. UNHCR.
United Nations High Commissioner for Refugees. (2025). Global Report 2024. UNHCR.
United Nations System Chief Executives Board for Coordination. (2021). Policy on the Organizational Resilience Management System. CEB.
United Nations System Chief Executives Board for Coordination. (2025). HLCM far-reaching efficiency initiatives. CEB.
World Food Programme. (2022). WFP Strategic Plan 2022-2025. WFP Executive Board.
World Food Programme. (2025c). WFP Strategic Plan 2026-2029. WFP Executive Board.
World Food Programme. (2025a). WFP Corporate Results Framework 2026-2029. WFP Executive Board.
World Food Programme. (2025b). WFP Innovation Strategy 2025-2027. WFP Executive Board.
World Health Organization. (2025a). WHO Health Emergencies: 2025 funding and priorities. WHO.
World Health Organization. (2025b). WHO’s Health Emergency Appeal 2025. WHO.