

NEW YORK CENTER FOR ADVANCED RESEARCH (NYCAR)
A Foundation Medicine Comprehensive Genomic Profiling Case Study
Master’s Research Publication
Research Publication by William I. Njemanze
Publication No.: https://doi.org/10.5281/zenodo.20448679
DOI: NYCAR-TTR-2026-RP024
June 2026
Peer Review and Publication Statement: Approved for NYCAR’s June 2026 publication release following review for applied healthcare scholarship, source discipline, APA 7th presentation, oncology-management relevance, diagnostic-governance clarity, model transparency, and professional readability. The main body is complete as submitted and requires no appendix material.
Abstract
Comprehensive genomic profiling has become part of advanced cancer care, but its clinical value is decided in a practical and often unforgiving sequence. The test has to be ordered early enough. The tissue has to be adequate. The report has to return before the treatment decision has already moved on. A molecular finding then has to be read correctly, paid for where coverage is required, explained to the patient, and connected to a therapy, trial, resistance interpretation, or a defensible decision to stay with standard care. When that sequence breaks, the science may still be sound while the patient gains little from it.
This paper uses Foundation Medicine’s FoundationOne CDx as a case study in comprehensive genomic profiling. The test is not examined as an endorsement, nor as a claim that one commercial platform defines precision oncology. Its public record is useful because it brings several live issues into one place: broad next-generation sequencing, companion-diagnostic use, tumor-signature reporting, variant interpretation, clinical report language, reimbursement, and the growing dependence of oncology teams on molecular evidence that must be translated under time pressure.
The evidence base includes FDA and CMS records, Foundation Medicine public documentation, ASCO and ESMO guidance, validation literature, and recent work on molecular tumor boards and implementation. The study follows the service pathway around the test: tissue handling, timing of the order, turnaround, variant review, molecular tumor board access, payer follow-through, clinical-trial referral, data stewardship, patient explanation, and equity across treatment settings. A weighted governance model is used to examine that pathway. It is not used to rank a company, validate a product, or predict survival.
The conclusion is practical. Genomic profiling improves advanced cancer care only when molecular evidence is tied to accountable clinical action. Late ordering, inadequate tissue, weak interpretation, delayed access work, unrealistic trial referral, and poor patient communication can turn a sophisticated laboratory result into information that arrives without force. Precision oncology therefore depends as much on governance, timing, and explanation as it does on sequencing.
Keywords: molecular pathology; precision oncology; Foundation Medicine; FoundationOne CDx; comprehensive genomic profiling; companion diagnostics; molecular tumor board; diagnostic governance.
Contents
List of Tables and Figures
Table 1. Comprehensive genomic profiling management chain.
Table 2. Precision oncology governance variables and weights.
Table 3. Implementation priorities for comprehensive genomic profiling.
Figure 1. FoundationOne CDx genomic scope.
Figure 2. Precision oncology governance pathway.
Figure 3. CGP governance score profile.
Figure 4. Weighted precision oncology governance model.
Figure 5. Access bottlenecks in comprehensive genomic profiling.
Figure 6. Molecular tumor board decision ecology.
Chapter 1: Introduction and Research Problem
Table 1. Comprehensive genomic profiling management chain
| Stage | Management responsibility | Risk if weak |
| Test ordering | Select suitable patient, timing, and specimen. | Testing occurs too late or without clinical purpose. |
| Laboratory processing | Protect tissue adequacy, tumor content, and analytical quality. | Result is delayed, failed, or incomplete. |
| Report interpretation | Connect variants with cancer context and treatment options. | Finding is misunderstood or ignored. |
| Molecular tumor board | Coordinate cross-specialist decision making. | Precision oncology becomes fragmented. |
| Access follow-through | Resolve coverage, trial referral, and patient communication. | Report fails to change care. |
Note. Original table prepared for NYCAR publication use. Copyright © June 2026 William I. Njemanze.
1.1 Cancer care after the single-marker era
Molecular pathology has moved oncology beyond the narrow habit of testing one alteration at a time after a treatment decision has already been made. Advanced tumors often contain several clinically relevant signals: driver alterations, resistance mechanisms, tumor mutational burden, microsatellite instability, copy number changes, and fusion events. Each signal may matter differently depending on tumor type, treatment history, specimen condition, and the patient’s remaining options. Comprehensive genomic profiling entered that environment not as an academic luxury, but as a response to a clinical workflow that had become too complex for scattered testing to manage well.
Foundation Medicine is a useful case because its products sit at the crossing point between laboratory science, oncology practice, regulatory approval, payer policy, and data interpretation. FoundationOne CDx does not simply produce a list of variants. It organizes molecular evidence into a report that clinicians must interpret against approved therapies, possible resistance, tumor-agnostic indications, and clinical trial opportunities. Any serious review has to examine the system around that report. A genomic result can be technically accurate and still fail the patient if tissue arrives late, if the result is not read by the right team, or if access work begins after treatment choices have narrowed.
Precision oncology often sounds elegant in conference language. Clinic work is less tidy. A patient may have progressive disease, limited tissue, declining performance status, insurance uncertainty, and a narrow window for next-line therapy. In that setting, genomic testing is not a ceremonial marker of modern care. It is useful only if it reaches the treating oncologist early enough to change a decision. Timing, specimen adequacy, interpretation, and payer follow-through become clinical management issues, not administrative side notes.
This study treats comprehensive genomic profiling as a diagnostic service rather than as a laboratory product alone. That distinction matters. Products can be purchased, ordered, and reported. Services require pathways, training, records, escalation rules, and accountability. Cancer centers that miss this distinction may celebrate access to advanced testing while leaving clinicians and patients to manage the difficult parts informally. NYCAR’s applied scholarship standard requires attention to that difference because public-facing research must be useful to decision makers, not only correct in terminology.
1.2 Research problem
Genomic testing has expanded faster than many clinical systems have matured. FDA-approved companion diagnostics, tumor-agnostic therapies, liquid biopsy options, and large-panel sequencing have widened what can be known about a tumor. Healthcare organizations, however, still face older problems: incomplete referrals, late orders, poor documentation, inequitable coverage, limited tumor board capacity, and uneven patient explanation. Those problems do not disappear because the test is sophisticated. They become more consequential because the information is more complex and often more time-sensitive.
Several management failures are especially damaging. Ordering may occur after multiple treatment lines have already failed. Pathology may not be consulted early enough to preserve tissue. Reports may be filed without structured review. Clinicians may see variants of uncertain significance without sufficient support. Payers may require documentation that delays action. Trial matching may remain theoretical because no one owns the referral. Data governance may be treated as an IT matter rather than a patient trust issue. Each weakness is familiar on its own; together they explain why molecular medicine can remain uneven despite technical progress.
Research on comprehensive genomic profiling frequently emphasizes analytic validity, actionability, or trial outcomes. Those topics are necessary, but they do not fully answer the management question. A health system also needs to know how genomic evidence travels through ordinary care. Who orders the test? Who checks tissue adequacy? Who explains the difference between an approved therapy and a possible trial? Who records why a result did not lead to treatment? Who notices whether uninsured, rural, older, or minority patients are tested later or less often? Without these questions, precision oncology remains professionally incomplete.
Central concern in this paper is therefore operational. Foundation Medicine’s case is used to ask how a molecular pathology service becomes dependable inside advanced cancer care. The point is not to promote one vendor or to imply that a single platform solves oncology. FoundationOne CDx offers a concrete case because it has public regulatory documentation, validation literature, and a visible role in companion diagnostics. That evidence allows the study to move beyond general praise and examine the working conditions required for responsible adoption.
1.3 Argument and contribution
Clinical value in comprehensive genomic profiling depends on four conditions. Ordering must be early enough to matter. Specimen handling must preserve the ability to generate a reliable result. Interpretation must connect molecular evidence with tumor context and therapeutic reality. Access work must move quickly enough to convert a possible option into care. Failure at any one point can weaken the whole chain. A report is not care until it has been interpreted, communicated, and acted on.
Foundation Medicine’s public profile is important, but the broader contribution of this paper lies in diagnostic governance. Governance is used here in a practical sense: who is responsible, what evidence is required, which deadlines matter, how decisions are documented, how fairness is assessed, and how the institution learns when a pathway breaks down. Molecular pathology brings a scientific foundation; governance determines whether that science reaches the patient in usable form.
Quantitative reasoning is used sparingly. A weighted governance model summarizes timing, specimen quality, interpretation, actionability, tumor board function, and equity. The score is not an estimate of patient survival, test accuracy, or company performance. It is a diagnostic management tool. Its value lies in making assumptions visible and forcing leaders to examine weak points before they become routine. A model of this kind belongs in applied healthcare management because it helps decision makers examine complex services without pretending that a single number settles clinical judgment.
Professional contribution also includes restraint. Genomic profiling can identify actionable findings, resistance information, and trial opportunities, but it cannot guarantee that a patient will receive a matched therapy. Biology, performance status, coverage, geography, trial eligibility, and patient preference still matter. Mature precision oncology respects that reality. It does not sell certainty; it builds a better pathway for uncertain but consequential decisions.
1.4 Research design and evidence discipline
Methodologically, the paper uses a qualitative-dominant case-study design supported by focused quantitative reasoning. That design fits the subject because comprehensive genomic profiling is not one event. It is a service pathway that includes ordering, specimen selection, laboratory processing, report interpretation, treatment access, patient communication, and follow-up. A purely numerical design would be misleading without internal patient-level data; a purely descriptive design would miss the need for management discipline.
Evidence comes from public regulatory records, Foundation Medicine product information, FDA and CMS material, peer-reviewed validation studies, ASCO and ESMO guidance, and recent literature on molecular tumor boards, implementation, equity, and clinical utility. No private patient files, invented interviews, or undocumented institutional statistics are used. That boundary is important. It keeps the paper honest and allows readers to check the foundation of the argument.
Case interpretation follows a simple rule: separate what is proven publicly from what must be governed locally. Public evidence can establish assay scope, approval history, validation claims, and policy environment. Local institutions still have to prove whether they order testing early, protect tissue, review reports, secure access, and communicate results well. The case therefore becomes a lens for practice rather than a claim that one company controls the future of oncology.
Academic contribution sits in that separation. The paper does not inflate comprehensive genomic profiling into a cure-all, and it does not dismiss its value because access remains uneven. Instead, it examines the space between scientific capability and clinical use. That is where many healthcare innovations either become dependable care or remain impressive but inconsistent technology.
Chapter 2: Comprehensive Genomic Profiling Literature
2.1 What comprehensive genomic profiling adds
Comprehensive genomic profiling adds breadth, but breadth is not the same as clinical value. The reason it matters in advanced solid tumors is that many treatment questions no longer sit neatly inside one gene, one drug, or one tumor type. A patient may need testing for an approved biomarker in the primary cancer, a resistance alteration after prior therapy, a tumor-agnostic marker, or a molecular signal that opens a trial rather than an immediate standard treatment. Single-gene testing can still be appropriate when the question is narrow. It becomes less efficient when the clinical problem is already wider than one alteration.
FoundationOne CDx is a useful case because it shows how comprehensive genomic profiling moved from specialist molecular pathology into routine oncology decision-making. FDA material identifies FoundationOne CDx as a tissue-based test that detects substitutions, insertion and deletion alterations, copy-number alterations, and selected rearrangements across 324 genes, along with selected genomic signatures relevant to solid tumors (U.S. Food and Drug Administration, 2024). The published validation work supports its role as a broad next-generation sequencing assay for solid tumors, while Foundation Medicine describes it publicly as a comprehensive genomic profiling test with companion-diagnostic uses (Foundation Medicine, 2026; Milbury et al., 2022). Those facts establish why the test belongs in a serious discussion of precision oncology. They do not settle whether the result will be ordered early, interpreted well, reimbursed smoothly, or connected to a realistic option for the patient.
The clinical question begins after the report is produced. A variant may be technically reportable and still have limited value for the person being treated. Some findings support an approved therapy in a specific tumor type. Some point toward tumor-agnostic treatment. Others help explain resistance, refine prognosis, or justify referral to a molecularly matched trial. Many findings sit in a more uncertain middle ground, where the oncologist has to weigh evidence strength, prior therapy, performance status, disease pace, access, and patient preference. ASCO’s provisional clinical opinion on somatic genomic testing in metastatic or advanced solid tumors is useful for that reason: it supports testing where results may guide care, but it does not treat genomic information as self-interpreting (Chakravarty et al., 2022).
Actionability needs discipline. The ESMO Scale for Clinical Actionability of Molecular Targets was developed because not every alteration deserves the same clinical weight. A target linked to a proven therapy in a defined setting is not the same as a biologically interesting alteration supported only by early evidence or trial rationale (Mateo et al., 2018). That distinction matters at the bedside. Patients may hear “mutation found” and assume a treatment has been found. Clinicians have to explain when a result is actionable, when it is uncertain, and when it does not change the immediate plan.
Comprehensive profiling also changes the work of pathology. Tissue becomes more than diagnostic material; it becomes a limited clinical resource. Tumor content, fixation, necrosis, decalcification, biopsy size, and prior tissue use can determine whether profiling succeeds or fails. If molecular testing is considered only after standard pathology has consumed the best material, the service may lose the evidence it later needs. In that sense, genomic profiling begins before the order is placed. It begins when tissue is obtained, handled, triaged, and protected for possible treatment decisions.
What comprehensive genomic profiling adds, then, is not only a larger panel. It adds a wider decision pathway. The test can bring therapy matching, resistance interpretation, trial referral, and tumor-signature assessment into one report. Its value depends on whether the oncology service can use that report without delay, exaggeration, or confusion. A broad molecular map helps only when the route from tissue to decision is organized well enough for the patient still to benefit.

Figure 1. FoundationOne CDx genomic scope. Copyright © June 2026 William I. Njemanze.
Source. FDA and Foundation Medicine public product information; original visualization prepared for NYCAR publication use.
2.2 Guidance, actionability, and evidence levels
ASCO’s provisional clinical opinion on somatic genomic testing in metastatic or advanced solid tumors supports genomic testing where biomarkers are linked to approved therapy, and it also recognizes the role of testing for tumor-agnostic indications and selected fusions. That guidance does not ask clinicians to test blindly. It asks them to connect molecular testing with therapeutic relevance. Such a position is important for management because it places responsibility on the care pathway, not only the laboratory.
ESMO’s ESCAT framework offers another useful discipline. By ranking genomic alterations according to clinical evidence, ESCAT helps distinguish findings with strong therapeutic support from signals that remain exploratory. Oncology practice needs that separation. Without it, patients may hear the word actionable when the practical next step is weak, unavailable, or unsupported by enough evidence. Precision medicine loses trust when it confuses biological interest with treatment readiness.
Molecular tumor boards have developed partly because interpretation is no longer a solo act. Pathologists, oncologists, geneticists, pharmacists, trial coordinators, and sometimes ethicists or payer specialists may need to review the same report. Westphalen and colleagues’ ESMO work on molecular tumor board structure and quality indicators reflects a growing recognition that decision quality depends on team process. Good boards do not merely admire rare variants. They decide whether a finding changes treatment, warrants a trial search, requires germline referral, or should be documented without immediate action.
Literature on implementation shows unevenness. Multicenter studies can demonstrate feasibility, high testing success, and treatment recommendations, yet actual receipt of matched therapy may remain lower than the number of actionable findings suggests. Reasons include patient deterioration, unavailable drugs, trial distance, coverage limits, and clinical judgment against treatment. Serious research should not hide this attrition. A useful paper should show where molecular promise narrows as it passes through real healthcare systems.
2.3 From analytic validity to diagnostic governance
Analytic validity asks whether the assay detects what it claims to detect. Clinical validity asks whether detected alterations have meaningful association with disease or therapy. Clinical utility asks whether testing improves patient management or outcomes. Governance asks a different but necessary question: can the institution make analytic and clinical value dependable across ordinary patients, not only in ideal cases? That final question is where health management enters the science.
FDA approval and validation studies establish a foundation. They cannot replace local workflow. Even a validated assay can be undermined by late ordering, inadequate documentation, poor report routing, or untrained interpretation. A laboratory report that arrives in an electronic record without an assigned reviewer may become a stranded object. A result requiring payer action may lose value if authorization work is delayed. Molecular data need a pathway with deadlines and owners.
Payer policy has shaped U.S. adoption of next-generation sequencing. CMS coverage decisions expanded access for eligible Medicare beneficiaries with advanced cancer, while local coverage policies and commercial payer rules continue to affect actual practice. Coverage language is not a dry reimbursement topic. In precision oncology, it determines who receives testing, when testing happens, and whether treatment can follow. Equity therefore begins inside policy and continues through every clinic step that translates policy into practice.
Implementation literature also warns against enthusiasm without audit. A center may report high test volumes while still missing patients who have poor referral access. Another may provide testing but fail to track whether reports lead to treatment, trial referral, or no action. Governance requires denominator discipline: eligible patients, tests ordered, tests completed, reports reviewed, options identified, options reached, and reasons for failure. Without denominators, precision oncology becomes a story of selected successes.
2.4 Economic evidence and clinical value
Cost discussion in precision oncology is often too narrow. Test price is easy to see, while the value of avoiding ineffective therapy, identifying a trial, clarifying resistance, or shortening diagnostic uncertainty is harder to measure. Economic evaluation therefore has to account for the whole care pathway. A report that arrives too late has little value even if the assay is scientifically impressive. A report that changes therapy at the right point may justify its cost through better sequencing of care, reduced waste, or improved patient planning.
Value also depends on disease setting. In tumors with well-established targetable alterations, comprehensive profiling may prevent a long sequence of scattered tests. In cancers with fewer validated targets, profiling may still support trial search or resistance interpretation, but expected clinical conversion may be lower. Treating all cancers as if they share the same genomic yield is poor management. Programs should review utilization by tumor type, stage, line of therapy, and action outcome.
Economic stewardship should not be confused with denial. A payer or administrator may reduce cost by limiting testing, but cost control that blocks appropriate testing can become clinically and ethically unsound. Likewise, unlimited testing without pathway control can waste resources. The better position is disciplined use: test when the result can plausibly change management, order early enough to matter, and track whether results lead to decisions.
Research centers should also examine opportunity cost. Every tumor board hour, pathology review, authorization appeal, and trial referral consumes professional time. If testing expands without staffing, the program may slow down the very care it intends to improve. Economic evidence therefore belongs with workforce planning, not only with reimbursement policy.
Chapter 3: Foundation Medicine Case Context
3.1 FoundationOne CDx as a case study
FoundationOne CDx is used here as a case because its public record is unusually visible. FDA device pages, Foundation Medicine product material, validation studies, and payer coverage history allow a structured analysis without relying on private company data. The test’s scope across 324 cancer-related genes, selected rearrangements, microsatellite instability, tumor mutational burden, and companion diagnostic claims makes it suitable for examining molecular pathology and care governance together.
Case-study use does not mean endorsement. Foundation Medicine is treated as an example of a broader transition: advanced cancer care is increasingly tied to large-panel genomic evidence. Other platforms, academic laboratories, and liquid biopsy services belong to the same landscape. FoundationOne CDx remains useful because it illustrates the practical consequences of moving from targeted tests to a broader report. More information can improve decisions; it can also create uncertainty if institutions do not know how to interpret and act on it.
Foundation Medicine’s portfolio also raises the tissue-versus-liquid question. Tissue-based testing remains central when adequate specimens are available. Liquid biopsy can help when tissue is limited, inaccessible, or when a rapid noninvasive option is clinically useful. Neither approach should be described as universally superior. Each has strengths, limits, and interpretation risks. Good governance tells clinicians when to use each option, how to explain negative results, and when repeat or complementary testing may be needed.
Advanced cancer patients do not experience product categories in the abstract. They experience waiting for a result, hearing whether a mutation has been found, learning whether insurance will pay, and facing whether treatment is possible. Case analysis therefore has to keep the patient pathway visible. FoundationOne CDx is technically important, but its public significance comes from how that technical capacity enters care.
3.2 Regulatory and coverage context
Regulatory approval gives clinicians a level of confidence that a test has been reviewed for intended use. FDA approval of FoundationOne CDx as a broad companion diagnostic placed comprehensive genomic profiling into a formal device framework for solid tumors. Later supplements and companion diagnostic additions show how the test’s clinical role changes as therapies and labels expand. That dynamic nature is central to precision oncology. A report environment can become outdated if it is not updated as evidence and drug approvals change.
CMS coverage policy also belongs in the case. National coverage for next-generation sequencing in advanced cancer created a route for eligible Medicare patients to receive tests meeting specified criteria. Coverage does not remove every access barrier, but it changes the management landscape. Clinicians, billing teams, navigators, and tumor boards must understand eligibility, documentation, and follow-through. Precision oncology governance therefore includes reimbursement literacy.
Commercial payer variation remains important. Patients outside Medicare may face prior authorization, denial, out-of-pocket exposure, or plan-specific restrictions. Rural practices may lack local expertise. Community oncology sites may depend on external pathways for molecular tumor board review. Academic centers may have better infrastructure but still struggle with speed and trial access. A responsible case study does not treat coverage as solved because one payer pathway exists.
Policy interpretation must remain current. New drug approvals, companion diagnostic claims, local coverage updates, and guideline revisions can change the meaning of a genomic result. Static protocols are risky in this field. Health systems need an update mechanism that links oncology, pathology, pharmacy, payer relations, and informatics. Without it, old pathways can continue to guide new science.
3.3 Case boundaries
Public evidence limits the paper’s claims. No internal Foundation Medicine records, hospital performance data, proprietary turnaround-time data, or patient-level outcomes are used. That boundary is deliberate. It protects the work from pretending to know what is not available. Public sources can support a governance analysis; they cannot prove how every institution orders, interprets, or acts on every test.
Scoring in the governance model is author-developed and interpretive. It reflects the case evidence and the management logic reviewed in the paper. It should not be read as a clinical outcome measure, company rating, or regulatory assessment. The numbers are meant to help readers see the pathway. They function like a management scorecard: useful for discussion, not definitive by themselves.
Foundation Medicine’s case also cannot represent every cancer type equally. Actionability varies widely by disease, stage, treatment history, tissue availability, and geography. Lung cancer, colorectal cancer, breast cancer, prostate cancer, melanoma, and rare tumors each carry different testing norms. A single paper cannot settle all of those clinical differences. What it can do is provide a governance lens that travels across settings.
Practical value lies in transfer. Hospital leaders, program directors, tumor board chairs, payer-access teams, and graduate researchers can use the case to ask whether their own pathway protects timing, tissue, interpretation, access, and equity. Transfer does not mean copying Foundation Medicine’s model. It means learning how a complex diagnostic service should be judged.
3.4 Report design and clinical readability
Report design carries clinical weight. A comprehensive genomic profile may include a large amount of molecular information, but clinicians need a hierarchy that separates urgent treatment signals from background findings. Report language should identify approved therapy associations, resistance implications, potential trials, tumor-agnostic markers, and uncertain findings without forcing the oncologist to reconstruct the evidence alone during a busy clinic day.
Readable reports do not mean simplified science. They mean disciplined presentation. Variant nomenclature, evidence level, therapeutic association, and limitations should be clear enough for oncologists, pharmacists, tumor boards, and navigators to use consistently. Poor presentation increases the risk that one clinician overacts, another ignores the same result, and a patient receives uneven advice depending on where the report lands.
Foundation Medicine has invested in report structure and therapeutic associations, yet institutional interpretation still matters. A commercial report cannot know every local formulary issue, trial slot, patient preference, insurance rule, or performance-status concern. Local governance therefore has to translate the report into a care decision. That translation is where molecular pathology, oncology, access work, and patient communication meet.
Clinical readability should be audited through user behavior. Programs can ask whether clinicians understand the report, whether tumor board notes clarify action, whether patients receive plain explanation, and whether access teams know which evidence to submit. Those questions turn report design from a vendor matter into a service-quality issue.
Chapter 4: Molecular Pathology and Diagnostic Governance
4.1 Specimen quality and tissue stewardship
Specimen quality is the first governance test. Before sequencing begins, tissue has already passed through biopsy decisions, fixation, processing, pathology review, and block selection. Small biopsies, decalcified specimens, necrosis, low tumor purity, and exhausted tissue can weaken or prevent molecular testing. These details may appear technical, yet they carry management consequences. A center that delays genomic planning may discover too late that no adequate specimen remains.
Pathologists occupy a central position in this chain. They know whether tissue is sufficient, which block is most suitable, whether macrodissection may help, and whether additional sampling is necessary. Oncologists often experience only the final report or failure notice. Governance connects those perspectives earlier. A good pathway should bring pathology into the decision before the last usable tissue is consumed by sequential tests or routine processing.
Specimen governance also requires language clinicians can use. Reports of quantity not sufficient, low tumor content, or assay failure should not end the conversation. They should trigger a defined response: review alternate tissue, consider liquid biopsy where appropriate, examine re-biopsy feasibility, and communicate the effect on treatment timing. Each step needs ownership. Otherwise, a failed test becomes a quiet delay rather than an active clinical problem.
Ethical stakes are real. Re-biopsy may create discomfort, cost, and risk for a patient who may already be medically fragile. Ordering must therefore be purposeful. A test that is unlikely to change management should not be presented as reflex modernity. Conversely, a patient with plausible targeted options should not lose opportunity because no one protected tissue early. Tissue stewardship is patient stewardship.
4.2 Report interpretation
Variant interpretation is where molecular pathology becomes clinical judgment. FoundationOne CDx and similar reports can identify short variants, copy number changes, rearrangements, tumor mutational burden, microsatellite instability, and therapeutic associations. Reading those findings requires more than recognition of a gene name. Tumor type, line of therapy, prior treatment, resistance context, evidence level, drug label, and trial availability all influence meaning.
Misinterpretation can occur in both directions. Some clinicians may overread variants and pursue weak options. Others may underuse a report because unfamiliar molecular language makes the finding seem remote from everyday oncology. Molecular tumor boards help by providing a structured setting for interpretation. Their value depends on discipline: clear cases, prepared summaries, evidence ranking, treatment feasibility, documentation, and follow-up.
Variants of uncertain significance require particular caution. They can be biologically interesting without being clinically actionable. Patient communication must avoid turning uncertainty into hope that the evidence cannot support. Precision oncology should be hopeful where evidence allows, but honest where evidence is immature. That balance is a professional skill, not a footnote.
Interpretation also affects institutional learning. If reports identify frequent barriers to action, the program should know. Are results arriving after treatment starts? Are actionable variants being missed because tumor board review is inconsistent? Are trial referrals failing because distance or eligibility rules intervene? Report interpretation should generate pathway intelligence, not only one-case decisions.
4.3 Tumor board practice
Molecular tumor boards are most useful when they convert complexity into accountable recommendations. A good board does not simply recite the report. It states whether the finding supports an approved therapy, an off-label discussion, trial referral, resistance interpretation, germline evaluation, or no immediate action. Documentation should include the reason. Without that record, future clinicians cannot easily understand why a genomic finding did or did not change care.
Membership matters. Medical oncology, pathology, molecular genetics, pharmacy, clinical trials, genetic counseling, nursing navigation, and payer access may all be relevant. Not every case needs every voice, but the system should know when to bring each function in. A tumor board that lacks access and trial coordination may generate recommendations that never reach the patient. A board without pathology may overlook specimen constraints. A board without documentation becomes institutional memory by rumor.
Turnaround time matters as much as expertise. A monthly tumor board may be educational but too slow for many advanced cancer decisions. Some centers use rapid virtual review, disease-specific molecular clinics, or structured electronic consultation. Format is less important than fit. Patients with active progression need a pathway that matches clinical urgency.
Governance should track board performance. Useful indicators include time from report receipt to review, percentage of reports reviewed, percentage with documented recommendation, number referred to trials, number receiving matched therapy, and reasons for nonaction. These indicators do not reduce care to metrics. They help leaders see whether the system is doing what it claims.
4.4 Companion diagnostics and resistance logic
Companion diagnostic status gives a molecular finding formal therapeutic relevance, but it should still be read in clinical context. A label-linked biomarker may point toward a treatment, yet prior exposure, comorbidity, organ function, performance status, and patient goals remain decisive. The test can identify eligibility; it cannot complete judgment. Governance protects that distinction.
Resistance interpretation has become increasingly important as targeted therapy moves earlier in care. A tumor may change under treatment pressure. New alterations may explain why a therapy stopped working or why a later option is unlikely to help. Comprehensive profiling can support this analysis, but only when clinicians order it at a relevant moment and compare findings with treatment history. Molecular data without a timeline is often less useful than it appears.
Tumor-agnostic indications add another layer. Markers such as microsatellite instability and tumor mutational burden may support treatment across cancer types under specified conditions. These markers should not be treated as slogans. Their predictive meaning depends on assay method, clinical setting, drug label, and evidence interpretation. Precision oncology is strongest when it respects both the promise and the boundary of tumor-agnostic treatment.
Pharmacists can help connect companion diagnostic findings to real treatment conditions. Dosing, interactions, toxicity, access restrictions, and sequencing concerns often determine whether an option is practical. Molecular tumor boards that include pharmacy input tend to make recommendations that are closer to usable care.
Chapter 5: Precision Oncology Operations
5.1 Ordering and turnaround
Ordering comprehensive genomic profiling is not a clerical step. It is a clinical timing decision. In metastatic or advanced disease, waiting until standard options are exhausted may reduce the chance that a patient remains well enough to benefit. Earlier testing, where clinically appropriate, gives oncologists more room to compare targeted therapy, immunotherapy markers, trial options, and resistance clues. Late testing often produces information after the decision window has closed.
Turnaround time should be managed from the moment the question arises, not from the day the laboratory accepts the specimen. Real delay includes recognition, consent if required, specimen request, pathology review, shipping, sequencing, report delivery, interpretation, payer review, and treatment access. Programs that count only laboratory processing time may underestimate what the patient experiences. Operational honesty requires measuring the full chain.
Electronic health records can help or hinder. A simple order set may improve consistency. Poorly designed workflows may bury results in scanned documents, place them outside oncology review, or fail to alert the right clinician. Informatics should be built around action: result received, interpretation pending, recommendation made, access step assigned, patient informed. Anything less leaves too much to memory.
Ordering discipline also protects against unnecessary testing. Some patients may not benefit because disease status, prior testing, performance status, or goals of care make the result unlikely to alter management. Clinical discretion should remain. Governance does not mean ordering every test; it means making the reason for ordering or not ordering explicit enough for professional review.
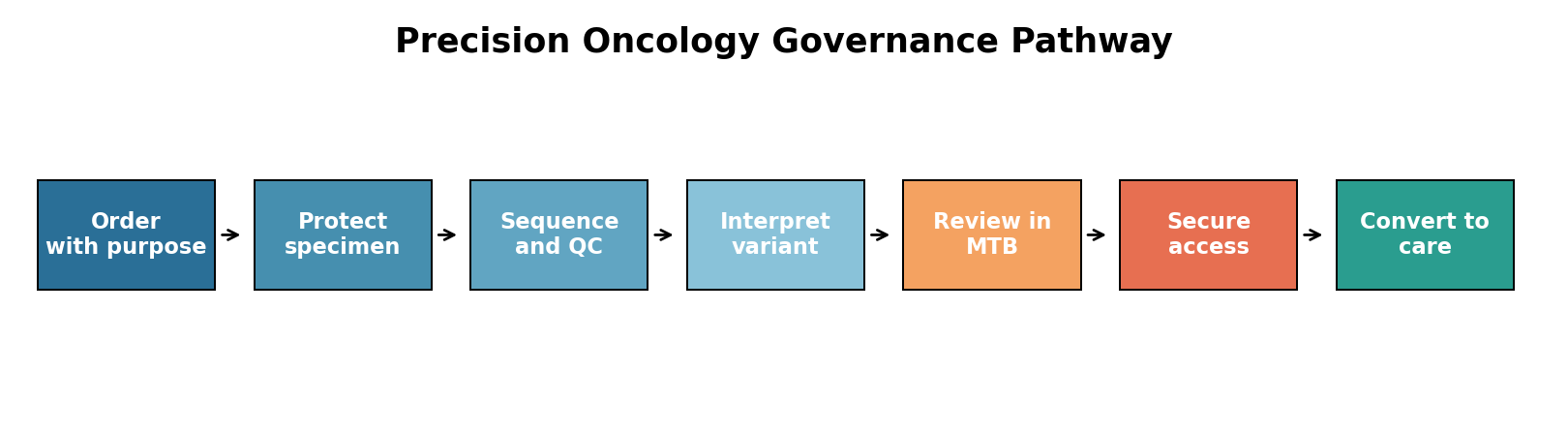
Figure 2. Precision oncology governance pathway. Copyright © June 2026 William I. Njemanze.
Source. Author-developed service pathway derived from the case analysis.
Read also: Behavioral Strategies In Health And Social Care Management
5.2 From report to treatment
Molecular reports often give several categories of information. Some findings point to FDA-approved therapies in the tumor type. Some point to tumor-agnostic indications. Others suggest resistance, prognosis, or clinical trials. The oncology team must sort those categories quickly. Treating every finding as equal slows the pathway and confuses communication. A structured interpretation note can separate immediate clinical action from longer-range information.
Payer access is part of treatment conversion. Prior authorization, evidence submission, formulary limits, and patient assistance may determine whether a recommendation becomes a prescription. Program leaders should not leave this work to improvisation after the tumor board has spoken. Access teams need early notification, documentation templates, and escalation rules. A genomic recommendation without access support is often a partial decision.
Trial matching is also vulnerable to attrition. A report may identify a plausible trial, but eligibility, geography, slots, biopsy requirements, travel, and patient preference may prevent enrollment. Tracking only potential matches exaggerates program impact. A more honest record follows the path from molecular finding to trial discussion, referral, screening, and enrollment or reason for non-enrollment.
Patient communication deserves more care than it often receives. Genomic reports can sound decisive, yet many findings are probabilistic or context-dependent. Patients need to understand whether a result opens a standard treatment, suggests a trial, explains resistance, or provides no immediate option. Plain language does not weaken scientific seriousness. It protects consent and trust.
5.3 Managing uncertainty
Precision oncology produces uncertainty as well as clarity. A result may identify no actionable alteration. A tumor may carry an alteration with evidence in another cancer type but not the patient’s own. A drug may be available only in a trial. A therapy may be biologically plausible but clinically weak. Governance should prepare clinicians to manage these outcomes without overpromising.
Negative results require explanation. A patient who undergoes comprehensive profiling may expect a targeted therapy. When none appears, the team should clarify that absence of an actionable alteration is still useful information, though not the desired result. It may prevent unsuitable treatment, support standard care, or guide future testing. Silence after a negative report can feel like abandonment.
Uncertainty also appears when tissue and liquid biopsy results differ. Clonal heterogeneity, tumor shedding, sampling site, treatment pressure, and assay limits may all matter. Clinicians need rules for reconciling discordant information. Those rules should draw on pathology, molecular expertise, and clinical context rather than a simplistic hierarchy.
Every precision-oncology program should build a feedback loop. Cases where results did not alter care are as important as successful matches. They reveal timing problems, access barriers, tissue failures, unrealistic trial pathways, and communication gaps. A program that learns only from successes will repeat avoidable failures.
5.4 Trial matching and sequencing discipline
Trial matching is not simply a search function. A trial option must be evaluated against eligibility, disease tempo, prior therapy, travel, insurance, patient preference, and urgency. Reports that list trial possibilities can be helpful, but they do not complete the work. Someone must decide whether the option is realistic and whether discussion should happen now or after another treatment step.
Sequencing discipline matters because targeted therapies can be lost through poor timing. If a patient receives a later-line standard regimen while a relevant genomic result sits unreviewed, the opportunity may narrow. If a trial is discussed only after performance status declines, referral may become symbolic. Care teams need rules for when genomic evidence should interrupt, redirect, or support the existing treatment plan.
Clinical trial offices should be linked to molecular review. Trial coordinators can confirm slot availability, screening requirements, geography, tissue needs, and timeline before a recommendation is given to the patient. Without that link, tumor boards may produce recommendations that sound promising but collapse during referral.
Patient preference remains central. Some patients may choose local standard care over travel for a trial. Others may accept travel if the rationale is explained clearly. Good governance does not pressure every patient toward research participation. It makes the option understandable and reachable when it is appropriate.
Chapter 6: Governance Model and Quantitative Reasoning
Table 2. Precision oncology governance variables and weights
| Variable | Meaning | Weight | Illustrative score |
| T | Test timing: order early enough to influence decision. | 0.18 | 76 |
| Q | Specimen quality: adequate tissue, tumor content, and assay success. | 0.16 | 82 |
| I | Interpretation quality: evidence ranking and report-to-decision clarity. | 0.22 | 86 |
| A | Action conversion: therapy, trial, resistance, or management decision reached. | 0.18 | 80 |
| C | Coordination: molecular tumor board and cross-functional follow-through. | 0.14 | 74 |
| E | Equity: access across payer, site, geography, and patient group. | 0.12 | 74 |
Note. G = 0.18T + 0.16Q + 0.22I + 0.18A + 0.14C + 0.12E = 79.36, rounded to 79. Original table prepared for NYCAR publication use. Copyright © June 2026 William I. Njemanze.
6.1 Model purpose and variables
Weighted reasoning is included to clarify the governance argument. It does not estimate survival, assay sensitivity, company quality, or population benefit. It asks a narrower management question: how strong is the pathway that moves comprehensive genomic profiling from order to usable care? Such a model is appropriate only when its limits are visible. Numbers help organize judgment; they do not replace it.
Model variables are deliberately plain. T represents test timing. Q represents specimen quality. I represents interpretation quality. A represents action conversion. C represents tumor board coordination. E represents equity and access. Each variable is scored from zero to one hundred. The overall governance score is calculated as G = 0.18T + 0.16Q + 0.22I + 0.18A + 0.14C + 0.12E. Interpretation receives the highest weight because report meaning is the hinge between laboratory output and treatment decision.
Author-developed values used for illustration are T = 76, Q = 82, I = 86, A = 80, C = 74, and E = 74. These values yield G = 79.4. Rounded to the nearest whole number, the governance score is 79 out of 100. The score indicates a mature but incomplete pathway: strong technical and interpretive capacity, with access, coordination, and timing still requiring management attention.
Healthcare organizations can adapt the model using its own data. Test timing could be measured through days from progression to order and days from order to report. Specimen quality could include failure rates and repeat biopsy rates. Interpretation quality could use tumor board review rates and documentation completeness. Action conversion could track matched therapy or trial referral. Equity could examine payer, site, race, geography, and age patterns.
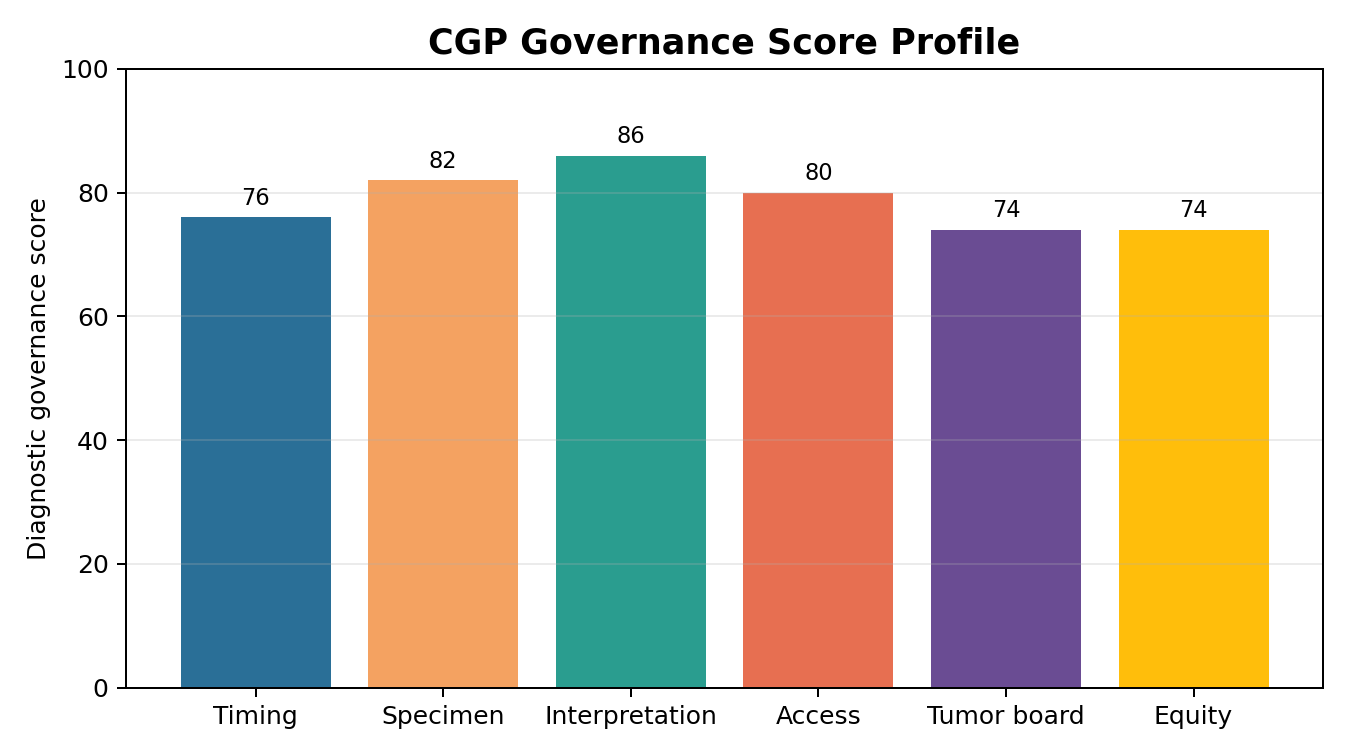
Figure 3. CGP governance score profile. Copyright © June 2026 William I. Njemanze.
Source. Author-developed diagnostic scoring for management discussion; not a clinical performance rating.
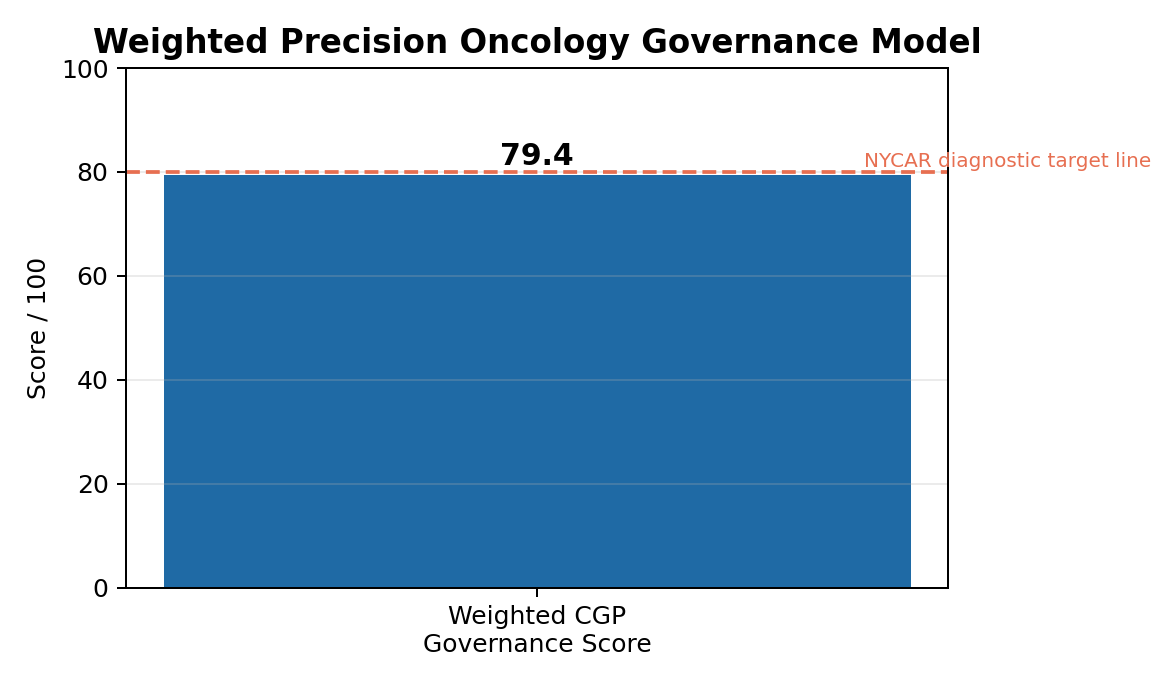
Figure 4. Weighted precision oncology governance model. Copyright © June 2026 William I. Njemanze.
Source. Computed from the author-developed weighted model.
6.2 Math check and interpretation
Arithmetic is straightforward. The timing contribution is 0.18 x 76 = 13.68. Specimen quality contributes 0.16 x 82 = 13.12. Interpretation contributes 0.22 x 86 = 18.92. Action conversion contributes 0.18 x 80 = 14.40. Tumor board coordination contributes 0.14 x 74 = 10.36. Equity contributes 0.12 x 74 = 8.88. Added together, the components equal 79.36, presented as 79.4 in the figure and rounded to 79 in narrative discussion.
Mathematical restraint is important. A score near 80 should not invite celebration without inspection. Interpretation may be strong while equity remains weak. Specimen handling may be reliable while trial access fails. A single total score can hide unevenness if leaders do not read the components. For that reason, the paper presents both the formula and the component profile.
Weight selection is also a judgment call. Another institution might weight equity higher because it serves a rural or historically underserved population. A center with repeated assay failures might weight specimen quality higher. A high-volume academic program might focus on tumor board throughput. The model’s value comes from making these decisions explicit. Hidden weights already exist in every program; the model forces them into discussion.
No p-values, confidence intervals, or regression claims are offered because the study does not use patient-level outcome data. Introducing statistical language without data would weaken the paper. Conceptual modeling is enough for this purpose. It gives administrators and clinicians a disciplined way to discuss a service that is clinically complex and operationally fragile.
6.3 Responsible use
Responsible use begins with denominators. Programs should know how many eligible patients were seen, how many were tested, how many tests succeeded, how many reports were reviewed, how many recommendations were made, and how many recommendations reached treatment or trial screening. Without denominators, precision oncology appears more successful than it may be in routine care.
Governance review should not be punitive. Delays and failures often reveal system design problems, not individual negligence. A pathologist may receive tissue late because ordering was late. An oncologist may not act because a result was routed poorly. A patient may miss a trial because transportation and insurance were not addressed early. Good review identifies the weak link and repairs the pathway.
Clinical judgment must remain central. Some patients should not pursue aggressive matched therapy because goals of care, performance status, toxicity, or personal preference point elsewhere. A pathway that turns every genomic finding into automatic treatment is not responsible. Governance protects decision quality by ensuring that action and nonaction are both reasoned and documented.
Comparative use across institutions should be cautious. Scores may reflect patient population, payer mix, data maturity, and service design. A community cancer center and an academic center may need different thresholds. The model should stimulate better questions, not produce a ranking table detached from context.
6.4 Sensitivity, thresholds, and limits
Sensitivity review keeps the model honest. If interpretation weight is reduced and equity weight is raised, the overall score changes only modestly, but the conversation changes sharply. Leaders begin to ask whether a technically sophisticated program is still failing patients who cannot reach timely testing or matched treatment. Such a shift is useful because it shows how values are embedded in weights.
Thresholds should be set by purpose. A research hospital may require a higher tumor board coordination score because it handles rare cancers and trial-heavy decisions. A community program may emphasize timing and access because delays and payer barriers are more visible. The model should be adjusted to fit institutional responsibility. Copying weights without reflection would make the tool mechanical rather than professional.
Limitations remain clear. A governance score cannot prove improved survival, response rate, or quality of life. Those outcomes require patient-level evaluation and long-term follow-up. The score only asks whether the service conditions are credible. In that sense, it functions like a readiness assessment: not the final proof of benefit, but a disciplined check on whether benefit can realistically reach patients.
Programs should also resist metric gaming. A center can improve apparent turnaround by excluding difficult cases, improve action rates by testing only obvious cancers, or improve equity reports by failing to collect demographic detail. Good governance anticipates these risks. Indicators should be reviewed by clinicians, administrators, and equity leads together, with enough narrative context to prevent superficial success.
Chapter 7: Equity, Data Stewardship, and Institutional Learning
7.1 Equity in testing and access
Precision oncology can widen or narrow disparities depending on how it is governed. Patients with better insurance, academic-center access, transportation, digital literacy, and specialist referral may reach genomic testing earlier. Patients in rural areas, low-resource systems, or fragmented coverage environments may wait longer or miss testing altogether. Equity is therefore not an optional social paragraph. It is part of diagnostic performance.
Coverage policy helps but does not settle fairness. Medicare coverage for eligible next-generation sequencing tests can improve access for certain patients, but commercial payer variation, documentation requirements, and site-level familiarity still matter. Staff who understand payer rules can prevent delay. Patients without such navigation may experience precision oncology as another barrier added to an already difficult diagnosis.
Race, ancestry, geography, and socioeconomic status also shape trial access. A molecular finding may point to a trial, but distance, eligibility criteria, trust, language, work responsibilities, and cost can prevent participation. Programs that record only trial matching miss the equity question. They should track whether referred patients actually screen and enroll, and why others do not.
Equity work should be practical. Reflex testing protocols, community oncology partnerships, tele-molecular tumor boards, patient navigation, plain-language materials, and coverage assistance can reduce variation. None of these steps is glamorous. They are the ordinary infrastructure of fair genomic care.
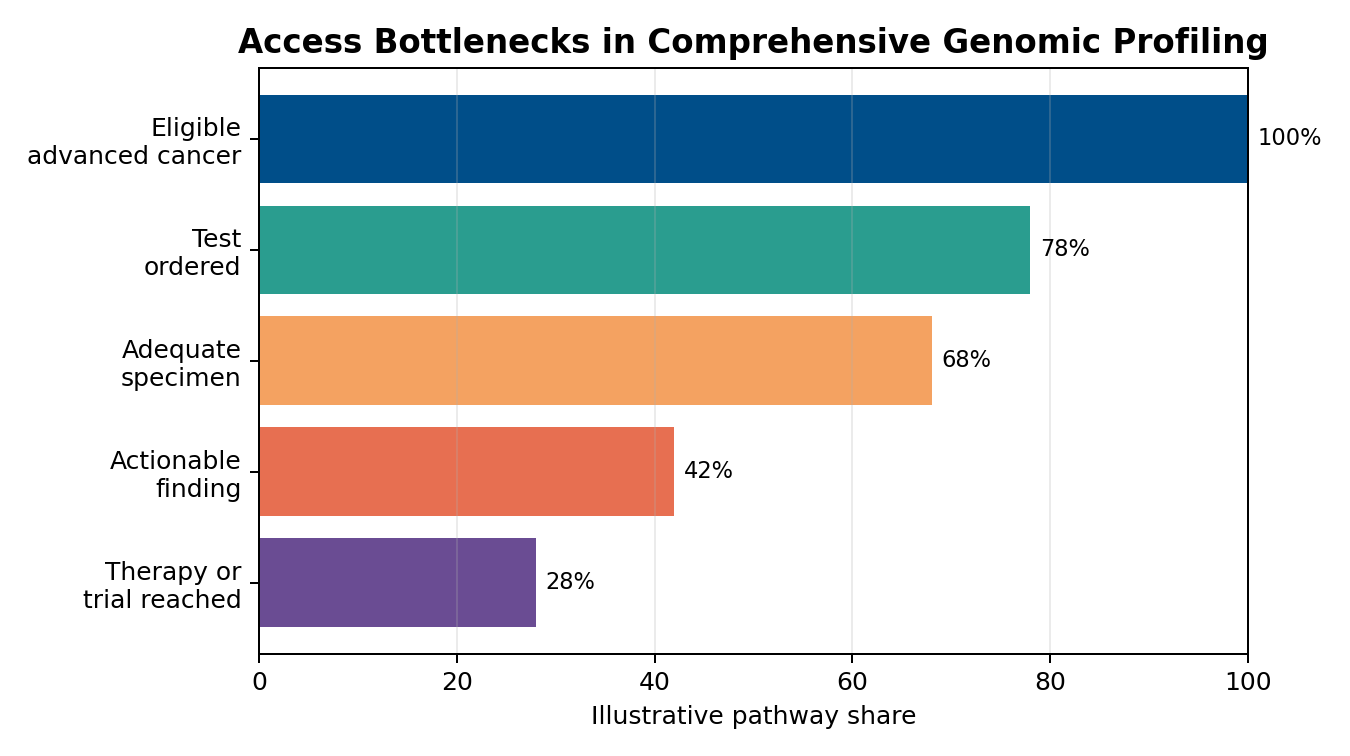
Figure 5. Access bottlenecks in comprehensive genomic profiling. Copyright © June 2026 William I. Njemanze.
Source. Author-developed illustration of common pathway attrition; not a patient-level dataset.
7.2 Genomic data stewardship
Genomic data carry clinical value and privacy risk at the same time. Tumor sequencing is usually somatic testing, yet reports may reveal findings with possible germline implications or family relevance. Data may also enter research, registries, vendor systems, or institutional analytics. Patients deserve clarity about how information is used, who can see it, and what happens when results suggest inherited risk.
Data stewardship should be built into the pathway rather than addressed only when a problem appears. Consent language, report storage, access controls, recontact policy, data-sharing rules, and audit trails require review. Oncology teams do not need to become privacy lawyers, but they do need enough understanding to answer patient questions honestly and direct concerns to appropriate support.
Artificial intelligence and decision-support tools will make data stewardship more important. As reports become more complex and algorithms assist interpretation, institutions must know how tools are validated, updated, and supervised. A decision-support prompt should not become hidden authority. Clinicians remain responsible for judgment, and systems remain responsible for the quality of tools placed in their hands.
Trust is fragile in cancer care. Patients may accept genomic testing because they hope it will improve treatment, not because they fully understand data flows. Institutions should not exploit that vulnerability. Plain explanation, careful records, and responsible data use are part of ethical precision oncology.
7.3 Learning from nonaction
Precision oncology programs often highlight successful matched treatments. Nonaction deserves equal attention. A report may fail to change care because tissue failed, the patient deteriorated, no actionable result was found, insurance delayed access, the trial was too far away, or the evidence was insufficient. Each reason teaches something different. Lumping them together as no action wastes learning.
Case review should distinguish unavoidable limits from fixable failures. Tumor biology may not offer a target. That is unavoidable. Late ordering, poor routing, missing authorization, and weak trial navigation are fixable. Programs should not comfort themselves with scientific uncertainty when operational delay was the real cause. Honest classification protects future patients.
Learning also requires humility. A matched therapy may produce little benefit. A patient may reject a recommendation. A trial may close. Real-world precision oncology is not a clean line from variant to response. Institutional learning should record outcomes without turning disappointment into blame. The aim is to improve the next decision, not to defend the last one.
Regular reporting can support the learning cycle. Quarterly reviews of test volume, turnaround, failed specimens, tumor board recommendations, access outcomes, trial referrals, and equity patterns would tell leaders whether the pathway is improving. Such reporting converts precision oncology from a specialty enthusiasm into a governed service.
7.4 Community oncology and referral equity
Community oncology settings carry much of the real burden of advanced cancer care. Many patients never enter a large academic center until late, if at all. Comprehensive genomic profiling must therefore work outside highly resourced institutions. If molecular tumor board access, tissue stewardship, and payer navigation exist only at academic sites, precision oncology will reproduce the geography of privilege.
Referral equity requires bidirectional design. Academic centers can support community clinicians through virtual review, shared pathways, rapid consultation, and trial-navigation assistance. Community clinicians can provide early patient context, local treatment history, and practical knowledge about travel, family obligations, and coverage barriers. Neither side owns the whole truth of the case.
Turnaround expectations should reflect community workflow. Specimen retrieval from outside pathology labs, prior authorization, and patient scheduling may take longer when systems are not integrated. Ignoring those delays creates unfair comparison. Improvement should focus on shared infrastructure: standard request forms, electronic report routing, and clear points of contact.
Equitable referral also means not transferring only the most complex administrative burden to the patient. A patient should not have to collect pathology slides, decode insurance letters, and identify trials alone. Navigation is not a luxury in this setting. It is the bridge between molecular possibility and usable care.
Chapter 8: Implementation Priorities
Table 3. Implementation priorities for comprehensive genomic profiling
| Priority | Action | Expected value |
| Early ordering | Define eligible settings and timing triggers. | Protects the clinical decision window. |
| Tissue stewardship | Add pathology review before order completion. | Reduces failed or delayed testing. |
| Interpretation workflow | Route reports to molecular review with evidence ranking. | Improves consistency and documentation. |
| Access navigation | Link payer support and trial referral to board recommendations. | Increases conversion from result to care. |
| Equity monitoring | Report testing and action rates by site, payer, and demographic pattern. | Detects hidden exclusion. |
Note. Original table prepared for NYCAR publication use. Copyright © June 2026 William I. Njemanze.
8.1 Ordering rules and specimen planning
Implementation should begin with clear ordering rules. Eligible disease settings, timing triggers, prior testing history, and tissue requirements should be written in language clinicians can use. Overly broad rules create waste and confusion. Overly narrow rules deny opportunities. Good rules support judgment while reducing avoidable variation.
Specimen planning should sit near the front of the pathway. When metastatic disease is diagnosed or progression occurs, oncology and pathology should know whether tissue is available, whether prior tissue is suitable, and whether re-biopsy or liquid biopsy should be considered. A simple specimen review step can prevent late failure. That step is especially important in cancers where small biopsies and limited tissue are common.
Consent and patient explanation should not be rushed. Patients need to know why testing is being ordered, what kinds of results may appear, why no actionable result is possible, and how long the process may take. Plain communication reduces unrealistic expectations and helps patients participate in decisions. Technical excellence without explanation is poor care.
Ordering metrics should include both speed and purpose. A center should not reward rapid testing if many orders are clinically irrelevant. Nor should it reward low utilization if eligible patients are being missed. Balanced review asks whether the right patients are tested early enough, with adequate tissue, and with a clear clinical question.
8.2 Tumor board and interpretation workflow
Interpretation workflow should be designed before the first report arrives. Reports should route automatically to the treating oncologist and the molecular review pathway. Cases with urgent or high-impact findings should have escalation rules. Clinicians should not have to search scattered files or rely on informal messages to know whether a result has been reviewed.
Molecular tumor board documentation should be concise and actionable. Recommended fields include diagnosis, stage, treatment history, specimen source, key alterations, evidence level, potential therapy, trial option, payer/access requirement, patient communication plan, and reason if no action is recommended. Such records support continuity when clinicians change or care transfers.
Board access should extend beyond academic centers where possible. Community practices may benefit from virtual molecular review or regional partnerships. Centralized expertise can reduce inequity if it is designed to include smaller sites. Without such support, genomic care may remain concentrated among patients who already have the strongest access.
Training should focus on practical interpretation. Clinicians do not need to memorize every alteration. They do need to understand actionability categories, resistance language, tumor-agnostic indications, uncertain findings, and when to consult pathology or genetics. Program maturity grows when frontline teams can recognize what they do not know early enough to seek help.
Figure 6. Molecular tumor board decision ecology. Copyright © June 2026 William I. Njemanze.
Source. Author-developed implementation map for NYCAR publication use.
8.3 Access, navigation, and patient follow-through
Access work should begin when a likely actionable route appears, not after a patient has waited through another appointment cycle. Prior authorization, appeal documentation, trial referral, travel support, financial counseling, and pharmacy review should be linked to the tumor board decision. A recommendation without navigation is not a complete service.
Patient navigators can protect continuity. They can help patients understand appointments, coverage letters, trial screening, specimen requests, and treatment scheduling. Navigation is especially important for patients with limited health literacy, language barriers, transport difficulties, or unstable insurance. Precision medicine should not require a patient to become a project manager while ill.
Follow-through metrics should be patient-facing. Did the result reach the oncologist? Was it explained? Was a recommendation recorded? Did access work start? Did the patient receive therapy, enter screening, or decline? Was the reason documented? These questions are more useful than counting tests alone.
Implementation also needs a stop rule. Not every genomic option should be pursued indefinitely. Toxicity, patient goals, evidence weakness, and clinical decline may make further pursuit inappropriate. Mature programs know when to act and when to protect the patient from burdensome escalation.
8.4 Quality indicators and audit practice
Quality indicators should be few enough to use and serious enough to matter. Recommended indicators include eligible-patient testing rate, median time from progression to order, median time from order to report, specimen failure rate, tumor board review rate, actionability category, matched therapy or trial referral rate, and documented reason for no action. These measures give leaders a practical view of the service.
Audit should include narrative review. Numbers may show that twenty patients did not reach matched therapy; narrative review explains why. Patient deterioration, no target, denial of coverage, travel barrier, trial closure, and clinical choice carry different meanings. Good audit separates fixable operational problems from biological and patient-centered limits.
Programs should review equity indicators at the same meeting where they review volume and turnaround. If one site orders tests late, if one payer group receives more denials, or if one demographic group is under-tested, the pathway needs correction. Equity belongs in quality management, not a separate annual statement.
Feedback should return to clinicians quickly. If pathology sees repeated inadequate specimens, oncologists need to know. If access teams see avoidable documentation failures, tumor boards need to adapt. If patients report confusion after result disclosure, communication materials need revision. Audit has value only when it changes behavior.
Chapter 9: Extended Professional Analysis
9.1 Foundation Medicine in the wider precision-oncology market
Foundation Medicine’s influence reflects a larger shift in oncology diagnostics. Laboratories now compete not only on analytic performance but on report design, companion diagnostic coverage, data integration, and clinician support. A report that is technically dense but clinically difficult to use may lose value. Vendors and institutions therefore share responsibility for making molecular evidence readable, current, and connected to care.
Commercial growth in genomic testing brings a risk of overextension. Marketing language can make comprehensive profiling sound universally decisive. Clinical practice is more limited. Many patients will not receive a matched therapy even after testing. Reasons may be biological, logistical, financial, or personal. A responsible research publication should state that clearly. Precision oncology is powerful when it finds a meaningful target, but not every tumor yields a usable answer.
FoundationOne CDx’s FDA-approved status gives it a formal role that many laboratory-developed tests do not share in the same way. Still, real-world practice involves multiple platforms. Academic centers may use institutional panels, community practices may use commercial send-outs, and some patients may receive liquid biopsy first. Governance principles should apply across platforms: order with purpose, protect sample integrity, interpret with evidence, manage access, and record outcomes.
Competition may also improve patient care if it forces clarity around turnaround, report quality, evidence updating, and affordability. Health systems should evaluate vendors through performance data and service fit, not branding alone. The relevant question is whether a platform helps the institution make better cancer decisions within its actual pathway.
9.2 Patient communication and clinical ethics
Patients often hear genomic testing through the language of hope. Hope has a place in cancer care, but it should not be used to cover uncertainty. Clinicians should explain that comprehensive profiling may find an approved option, a clinical trial, resistance information, hereditary implications, or no immediate target. Each possibility should be understandable before testing begins.
Communication after the result requires the same care. A targetable alteration is not the same as a guaranteed response. A trial option is not the same as enrollment. A variant of uncertain significance is not a hidden cure waiting to be unlocked. These distinctions can be painful, but they protect the patient’s right to informed choice. They also protect clinicians from replacing evidence with optimism.
Family implications deserve careful handling. Although tumor profiling is usually performed to guide cancer treatment, some findings may raise concern for inherited risk. Clear referral pathways to genetic counseling should be available. Oncology teams should not leave patients with ambiguous statements about family risk without support.
Ethics also includes burden. Re-biopsy, travel for trials, out-of-pocket costs, and complex administrative steps may be hard for a patient with advanced disease. A recommendation should be judged not only by molecular logic but by feasibility and patient values. Precision care becomes humane when it respects the person carrying the tumor.
9.3 Institutional accountability
Hospital leaders should treat comprehensive genomic profiling as a service line with accountability. That does not mean turning every molecular decision into bureaucracy. It means recognizing that fragmented responsibility creates hidden failure. Pathology, oncology, finance, trials, pharmacy, data governance, and patient navigation all touch the pathway. Leadership must make their connection visible.
Budget review should include downstream effects. Testing has a price, but so do failed tissue use, delayed therapy, unnecessary treatment, repeated appointments, missed trials, and inequitable care. A narrow cost view may reject a test without seeing the cost of ignorance. A careless utilization view may order testing without regard for value. Financial stewardship requires a balanced frame.
Workforce capacity matters. Molecular tumor boards, pathology review, genetic counseling, authorization, and trial coordination all require skilled labor. Programs that expand testing without staffing interpretation and access will create bottlenecks. Technology does not remove professional work; it changes the kind of work needed.
Accountability should reach the boardroom in major cancer centers. Genomic medicine affects reputation, quality, equity, research participation, and patient trust. Senior leaders should know whether the pathway works, where it fails, and how improvement is being measured. Precision oncology is too consequential to remain a specialist concern hidden inside departmental routines.
9.4 Emerging tools and future risk
Emerging decision-support tools will change how genomic reports are read. Software may rank variants, suggest trials, identify drug associations, or flag germline concern. These tools can help busy clinicians, but they also create a new governance burden. Leaders must know how recommendations are generated, updated, and reviewed. No algorithm should quietly become the physician of record.
Artificial intelligence may improve literature matching and trial search, yet it can also reproduce bias if trained on incomplete data or if access assumptions are not examined. A trial recommendation that ignores geography, language, payer restrictions, or patient frailty may look technically sophisticated while remaining clinically unrealistic. Future precision-oncology governance must include fairness checks inside decision support.
Data interoperability will also matter. Genomic reports, pathology systems, oncology notes, pharmacy records, trial databases, and payer documentation often sit in separate places. Integration can reduce delay, but integration without governance can spread errors quickly. A wrong diagnosis, outdated variant interpretation, or poorly mapped report field may travel across systems before anyone notices.
Future risk is not only scientific. It is managerial. Programs may accumulate testing volume faster than they build interpretation capacity. Vendors may update reports faster than local protocols change. Payers may alter coverage faster than clinicians can track. Sustainable precision oncology will require institutions that can revise pathways without losing control of daily care.
9.5 Scenario testing for program maturity
Scenario testing can reveal whether a precision-oncology program is ready for real pressure. One useful scenario is the patient with newly progressed metastatic lung cancer, limited tissue, and a fast treatment decision pending. The program should be able to show how tissue is reviewed, whether liquid biopsy is considered, how quickly results route to oncology, and who begins access work if an actionable driver appears.
Another scenario involves a rare tumor with no standard targeted option but a possible trial signal. Here, maturity depends on trial-search discipline, evidence ranking, patient communication, and honest feasibility review. A program that merely lists distant trials without helping the patient understand eligibility and travel burden is not providing meaningful trial matching. It is outsourcing complexity to the patient.
One scenario involves an apparently negative report. Mature programs do not treat this as a dead end. They ask whether the specimen was adequate, whether prior treatment or tumor evolution suggests repeat testing later, whether standard care remains best, and how the result should be explained. Negative genomic information can still improve care when it prevents unrealistic treatment pursuit or clarifies the next conventional decision.
Scenario testing should become part of quality review. It forces teams to walk through the actual steps of care, including delays and handoffs that ordinary dashboards may hide. Leaders learn quickly whether their pathway depends on named individuals, informal texting, or institutional memory. Dependable precision oncology cannot rely on hidden favors. It needs a route that still works when the usual expert is absent.
Chapter 10: Recommendations and Final Position
10.1 Recommendations for clinical leaders
Cancer programs should create a written comprehensive genomic profiling pathway that begins before test order and ends only after a documented clinical decision. The pathway should specify eligibility, ordering triggers, specimen review, expected turnaround, report routing, tumor board criteria, access steps, patient communication, and outcome recording. A pathway that stops at report receipt is incomplete.
Pathology and oncology should review tissue stewardship together. Early block selection, tissue conservation, and contingency planning for inadequate specimens should become routine. Centers should monitor assay failure, repeat biopsy, and time lost to specimen problems. These data will show whether specimen quality is being managed or merely hoped for.
Molecular tumor board recommendations should use evidence levels and clear action categories. Approved therapy, trial option, resistance interpretation, germline referral, and no immediate action should be separated. Documentation should include why a recommendation was or was not pursued. Such clarity protects continuity and reduces confusion.
Equity indicators should be reported with the same seriousness as volume indicators. Testing rates by site, payer, geography, race, age, and language access can reveal hidden disparity. When inequity appears, leaders should respond with navigation, community partnerships, tele-review, coverage support, and clinician education.
10.2 Recommendations for payers and administrators
Payers should recognize that genomic testing decisions are time-sensitive in advanced cancer. Authorization rules that require excessive documentation or repeated appeals can turn a clinically relevant test into a late result. Coverage policy should protect appropriate use while reducing administrative delay for evidence-supported indications.
Administrators should fund interpretation and navigation, not only testing. A budget that pays for sequencing but not for tumor board time, authorization support, trial coordination, or patient explanation will produce an incomplete service. Precision oncology requires human infrastructure. Cutting that infrastructure weakens the value of the test.
Data systems should support action. Report status, review date, recommendation, access step, trial referral, and outcome should be visible to the care team. Dashboards should not be decorative. They should identify cases at risk of delay and assign responsibility for the next step.
Procurement should evaluate vendors through service performance: validation, regulatory status, report clarity, evidence updating, turnaround, support, data governance, and affordability. Brand visibility should not replace disciplined review. A genomic platform is only as useful as the clinical pathway it can serve.
10.3 Final position
Comprehensive genomic profiling has changed advanced cancer care by giving clinicians a broader view of tumor biology. Foundation Medicine’s FoundationOne CDx case shows why that change is significant. A single assay can organize information that once required scattered testing, and it can connect patients to approved therapies, resistance clues, immunotherapy markers, and trial possibilities. Scientific value is real.
Practical value remains conditional. Genomic testing helps patients when ordered in time, performed on adequate tissue, interpreted by capable teams, supported by payer and trial pathways, explained plainly, and reviewed for equity. Weakness at any point can turn a sophisticated report into a missed opportunity. That is the central management lesson of the case.
NYCAR’s publication standard is met here through source discipline, operational relevance, restrained claims, verified references, transparent modeling, and professional use value. The paper does not call genomic testing miraculous, and it does not reduce precision oncology to cost control. It treats comprehensive genomic profiling as a serious diagnostic service that demands clinical judgment and institutional responsibility.
Future cancer programs will be judged not by whether they can order genomic reports, but by whether those reports improve decisions for real patients under real constraints. Precision oncology will mature when institutions can explain who was tested, who was missed, what was found, what was done, what failed, and what changed afterward. That is where molecular pathology becomes accountable care.
10.4 Use in professional training and institutional review
Professional training should use comprehensive genomic profiling as a cross-disciplinary case. Pathology learners need to see how tissue choices affect treatment. Oncology learners need to understand evidence levels and report limits. Health-management learners need to examine payer policy, workflow, data stewardship, and equity. Precision oncology is too interconnected for single-discipline teaching.
Institutional review should revisit the pathway at least twice a year. Drug labels, companion diagnostic claims, local coverage rules, clinical trials, and guideline recommendations change. A program that was sound in January may be outdated by September. Scheduled review protects patients from stale practice and protects clinicians from relying on memory in a rapidly changing field.
Board-level summaries should be concise but candid. Leaders should see testing volume, turnaround, failures, action categories, access outcomes, trial referrals, equity signals, and improvement actions. Such reporting does not need to expose private patient details. It needs to show whether the service is functioning as promised.
Final value of the case lies in its demand for seriousness. Comprehensive genomic profiling is not a symbol of modern oncology unless it improves the work of care. Foundation Medicine’s case helps reveal what that work requires: science, timing, tissue, interpretation, access, communication, and institutional memory. When those elements are governed together, molecular pathology becomes more than a report; it becomes a disciplined route to better decisions.
10.5 Closing governance statement
Molecular medicine will keep expanding. More targets, more drug combinations, more resistance patterns, more blood-based assays, and more algorithmic interpretation will enter practice. Complexity will not decline. Care quality will depend on whether institutions make the pathway clearer as the science becomes richer. That is the central governance demand of precision oncology.
Foundation Medicine’s case helps illustrate a broader truth: diagnostic innovation is not finished at approval, validation, or report delivery. The work continues through specimen handling, interpretation, access, explanation, treatment, trial referral, documentation, and review. Each step is ordinary enough to be overlooked and important enough to determine whether a patient benefits.
For health leaders, the professional obligation is plain. Do not mistake a genomic report for precision care. Build the pathway that lets the report matter. Assign owners, measure delays, protect tissue, support tumor boards, watch equity, explain uncertainty, and learn from nonaction. When those duties are taken seriously, comprehensive genomic profiling earns its place in advanced cancer management.
William I. Njemanze’s research publication therefore closes with a practical standard. Precision oncology should be judged by the quality of decisions it enables for patients facing real disease pressure. Molecular pathology supplies the evidence. Governance determines whether the evidence arrives in time, is understood properly, and becomes care rather than another document in the record.
Sustainable practice also requires humility. Some cancers will not reveal a useful target. Some patients will be too ill for a trial or a new therapy. Some findings will remain uncertain even after expert review. A serious program acknowledges these limits without retreating from the work. It protects the patient from false certainty, protects the clinician from unstructured complexity, and protects the institution from mistaking technological access for clinical responsibility.
NYCAR’s standard for this publication is therefore practical as well as academic: the work must be traceable, current, useful, and readable by professionals who make decisions. Comprehensive genomic profiling deserves that level of discipline because it sits close to moments of real consequence. A patient waiting for the next cancer decision needs more than an impressive assay. The patient needs a system capable of turning evidence into a responsible next step.
Responsible care finally depends on continuity. Genomic knowledge should not disappear when a clinician leaves, when a report is scanned into the wrong part of the record, or when an authorization appeal is handled by a different office. The pathway has to preserve memory, ownership, and explanation. In advanced cancer, time is not a neutral resource. Governance matters because delay has clinical meaning.
References
Chakravarty, D., Johnson, A., Sklar, J., Lindeman, N. I., Moore, K., Ganesan, S., Lovly, C. M., Perlmutter, J., Gray, S. W., Hwang, J., Lieu, C., André, F., Azad, N., Borad, M., Tafe, L., Messersmith, H., Robson, M., & Meric-Bernstam, F. (2022). Somatic genomic testing in patients with metastatic or advanced solid tumors: ASCO provisional clinical opinion. Journal of Clinical Oncology, 40(11), 1231-1258. https://doi.org/10.1200/JCO.21.02767
Centers for Medicare & Medicaid Services. (2018). National coverage determination for next generation sequencing for Medicare beneficiaries with advanced cancer (CAG-00450N). https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?NCAId=290
Foundation Medicine. (2026). FoundationOne CDx product information. https://www.foundationmedicine.com/test/foundationone-cdx
Foundation Medicine. (2026). FoundationOne Liquid CDx product information. https://www.foundationmedicine.com/test/foundationone-liquid-cdx
Gueye, A., Maroun, B., Zimur, A., Berkovits, T., & Tan, S. M. (2024). The future of collaborative precision oncology approaches in sub-Saharan Africa: Learnings from around the globe. Frontiers in Oncology, 14, Article 1426558. https://doi.org/10.3389/fonc.2024.1426558
Mateo, J., Chakravarty, D., Dienstmann, R., Jezdic, S., Gonzalez-Perez, A., Lopez-Bigas, N., Ng, C. K. Y., Bedard, P. L., Tortora, G., Douillard, J. Y., & Andre, F. (2018). A framework to rank genomic alterations as targets for cancer precision medicine: The ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Annals of Oncology, 29(9), 1895-1902. https://doi.org/10.1093/annonc/mdy263
Milbury, C. A., Creeden, J., Yip, W. K., Smith, D. L., Pattani, V., Maxwell, K., Sawchyn, B., Gjoerup, O., Meng, W., & Skoletsky, J. (2022). Clinical and analytical validation of FoundationOne CDx, a comprehensive genomic profiling assay for solid tumors. PLOS ONE, 17(3), e0264138. https://doi.org/10.1371/journal.pone.0264138
National Cancer Institute. (2024). Precision medicine in cancer treatment. https://www.cancer.gov/about-cancer/treatment/types/precision-medicine
U.S. Food and Drug Administration. (2024). FoundationOne CDx (F1CDx) – P170019/S048. https://www.fda.gov/medical-devices/recently-approved-devices/foundationone-cdx-f1cdx-p170019s048
Volders, P. J., Aftimos, P., Dedeurwaerdere, F., Martens, G., Canon, J.-L., Beniuga, G., Froyen, G., Van Huysse, J., De Pauw, R., Prenen, H., Lambin, S., Decoster, L., Vaeyens, F., Rottey, S., Van Dam, P.-J., Rutten, A., Schreuer, M., Loontiens, S., Smeets, F., & Maes, B. (2025). A nationwide comprehensive genomic profiling and molecular tumor board platform for patients with advanced cancer. npj Precision Oncology, 9, Article 66. https://doi.org/10.1038/s41698-025-00858-0
Westphalen, C. B., Boscolo Bielo, L., Aftimos, P., Beltran, H., Benary, M., Chakravarty, D., Collienne, M., Dienstmann, R., El Helali, A., Gainor, J., Horak, P., Le Tourneau, C., Marchiò, C., Massard, C., Meric-Bernstam, F., Pauli, C., Pruneri, G., Roitberg, F., Russnes, H. E. G., Solit, D. B., Starling, N., Subbiah, V., Tamborero, D., Tarazona, N., Turnbull, C., van de Haar, J., André, F., Mateo, J., & Curigliano, G. (2025). ESMO Precision Oncology Working Group recommendations on the structure and quality indicators for molecular tumour boards in clinical practice. Annals of Oncology, 36(6), 614-625. https://doi.org/10.1016/j.annonc.2025.02.009
Woodhouse, R., Li, M., Hughes, J., Delfosse, D., Skoletsky, J., Ma, P., Meng, W., Dewal, N., Milbury, C., & Clark, T. A. (2020). Clinical and analytical validation of FoundationOne Liquid CDx, a novel 324-gene cfDNA-based comprehensive genomic profiling assay for cancers of solid tumor origin. PLOS ONE, 15(9), e0237802. https://doi.org/10.1371/journal.pone.0237802
World Health Organization. (2020). WHO report on cancer: Setting priorities, investing wisely and providing care for all. https://www.who.int/publications/i/item/9789240001299