

Building People-Centered, Climate-Ready Systems for Small-Island Futures
Research Publication by Favour I. Onyebuchi
Health Administration and Social Sciences in the Caribbean
New York Center for Advanced Research (NYCAR)
Date: June 2026
Publication No.: NYCAR-TTR-2026-RP058
DOI: https://doi.org/10.5281/zenodo.20630497
Peer Review and Publication Status:
This research publication has been reviewed under the editorial framework of the New York Center for Advanced Research. The review assessed source integrity, methodological coherence, originality of analysis, APA citation discipline, formatting quality, and suitability for public release. The work meets NYCAR’s master’s-level publication standard and is approved for research publication.
Copyright © June 2026 Favour I. Onyebuchi. All rights reserved.
Table of Contents
Abstract
Small-island health systems in the Caribbean carry a heavy administrative load. They must protect primary care, hospital continuity, medicine supply, public-health surveillance, workforce stability, and emergency response while working with small budgets, limited specialist pools, migration pressure, climate shocks, and a high burden of chronic disease. This study examines health administration in that setting as a practical field of public management shaped by social behavior, household hardship, trust, culture, geography, and regional cooperation. It uses documentary analysis of recent public evidence from PAHO, CARPHA, CARICOM, the World Bank, UNICEF, and WHO, with attention to noncommunicable disease care in the Eastern Caribbean, Trinidad and Tobago’s health-planning context, regional open-data work, climate and health country profiles, and the everyday demands placed on community-level services. No interviews, patient records, or private datasets are claimed. The central finding is direct: Caribbean health development will depend on better routines, not louder reform language. Primary care must track patients across time, data systems must help managers see risk earlier, social science must guide outreach and communication, regional procurement must reduce avoidable supply pressure, and workforce planning must treat retention as a development issue. The Caribbean does not need a copied large-state model. It needs shared capacity where scale is too small, local trust where care is delivered, and administrative discipline that protects patients before, during, and after crisis.
Keywords:
Caribbean health administration; social sciences; public health management; small island developing states; primary health care; noncommunicable diseases; climate and health; digital health; community trust; regional cooperation.
Method and Source Discipline
This study is grounded in documentary analysis. It does not draw on field interviews, private institutional data, or unpublished ministry records, and it makes no claim to do so. That choice was deliberate. The aim was to work rigorously within what is publicly available, treating the body of recent material produced by PAHO, CARPHA, CARICOM, the World Bank, WHO, and UNICEF as a serious and substantive evidence base in its own right. Sources were not collected broadly and filtered later. They were selected because each one speaks directly to at least one of five concerns that run through the study from beginning to end: chronic disease continuity, primary care organization, climate and health resilience, health information use, workforce pressure, and regional cooperation.
Reading that material carefully requires a particular kind of discipline. Public reports carry authority, but they also carry ambiguity. A regional strategy document describes where a health system intends to go. It does not confirm that the journey has been made. A policy framework can be technically sound, widely endorsed, and still only partially implemented three years after its launch. This study treats that gap between policy and practice as one of the central problems of Caribbean health administration, not as a footnote. Public documents are therefore read as evidence of direction, pressure, and priority rather than as proof of delivery. The distinction is not pedantic. A chronic disease patient navigating a referral pathway, a nurse managing a clinic with inadequate supplies, a health information officer trying to extract usable data from a fragmented system, none of them are served by a study that mistakes a published target for an achieved outcome.
The analytical lens applied throughout is a service pathway lens. Every piece of evidence is read against a consistent set of practical questions. Does this reform change how a patient moves through care? Does it reduce the friction that frontline staff absorb daily? Does it give administrators earlier, more reliable knowledge of where the system is under strain? That framing keeps the analysis close to the ground even when the sources being examined operate at the level of regional policy or international guidance.
The limitation of this approach deserves honest acknowledgement rather than defensive qualification. Documentary analysis, however disciplined, cannot reach inside a district health office, a rural clinic, or a household in the days before a hurricane makes landfall. The decisions made in those spaces, by people with direct knowledge of local conditions, local relationships, and local constraints, are not fully visible in any public report. What can be inferred from patterns across documents is not the same as what can be learned from sustained engagement with the practitioners and patients who carry these systems on their backs every day. This study does not pretend otherwise. It is precisely that gap between published evidence and lived practice that makes the case, argued in the final chapter, for future research grounded in frontline experience and community-level inquiry. The public record is a starting point. It is not a substitute for the knowledge that exists only in the field.
Chapter 1: Introduction
Figure 1. People-centered Caribbean health administration pathway. Source: Author synthesis from PAHO, CARPHA, World Bank, and WHO evidence. Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Across the Caribbean, health administration carries a burden wider than the running of clinics, hospitals, and ministries. Administrators must protect care delivery during hurricanes, manage the cost and timing of imported medicines, support professionals who work in small labor markets, and respond to diabetes, hypertension, cardiovascular disease, cancer, mental distress, injuries, and infectious threats. Behind each task sits a social question. People decide whether to seek care, trust advice, complete treatment, accept prevention messages, change diet, attend screening, or share information according to culture, income, family structure, belief, geography, and their previous experience with institutions.
A Caribbean approach to health administration therefore has to join management science with social science. Budgets, procurement, staffing rosters, medical records, epidemiological dashboards, and health laws matter. None of them works well where communities feel unheard, poor households cannot absorb indirect costs, patients lack transport, stigma blocks disclosure, or professionals leave because the system cannot offer career development. Health development is not a technical exercise alone. It is an administrative and social undertaking that has to respect small-island constraints while refusing small-island resignation.
Recent evidence makes the urgency clear. PAHO’s 2024 report on leading causes of death and disease burden in the Americas states that noncommunicable diseases and external causes dominate death and disability across the region, with NCDs producing a mortality rate of 412 per 100,000 people in 2019 and total deaths rising by 31 percent from 2000 to 2019 (Pan American Health Organization [PAHO], 2024a). Those figures sit behind a familiar Caribbean story: more people are living longer, but many are living with chronic conditions that require continuity, medicine, behavior change, screening, and family support.
Climate risk widens the task. PAHO, WHO, and UNFCCC launched seven Caribbean climate and health country profiles in 2026 for Belize, Guyana, Haiti, Jamaica, Saint Kitts and Nevis, Saint Lucia, and Trinidad and Tobago (PAHO, 2026). The profiles emphasize extreme heat, floods, vector-borne disease, food insecurity, early warning systems, intersectoral coordination, climate finance, and resilient health infrastructure. For a health administrator, those are not abstract environmental concerns. They shape ambulance access, medicine storage, dialysis continuity, maternal services, surveillance, public communication, and the safety of older people during extreme weather.
A useful starting point is to treat health administration as the discipline that turns public purpose into dependable service. In the Caribbean, that task has to be performed in settings where scale is limited, informal relationships matter, and a regional event can quickly become a national health emergency. Administrators must understand communities as carefully as they understand budgets. A plan that works on study but ignores transport, trust, food access, family care, and local authority will not travel far beyond the ministry building.
The Caribbean is not presented as a single uniform unit. Jamaica, Trinidad and Tobago, Haiti, Belize, Guyana, Saint Lucia, Grenada, Dominica, Barbados, and other territories differ in political history, financing, geography, and institutional capacity. Still, many of their health-administration problems share a family resemblance: small workforces, external shocks, chronic-disease pressure, and the need for regional cooperation. The analysis therefore uses regional patterns while respecting local variation.
The study’s contribution is practical. It argues that the next stage of Caribbean health development must give equal weight to administration, social science, and climate readiness. Technical reforms that ignore household behavior will fail quietly. Community projects that ignore budgeting and supervision will lose strength. Regional plans that do not improve the daily patient pathway will remain impressive documents rather than lived improvement. A serious Caribbean model has to hold these realities together.
The introduction also needs to clarify what development means in this setting. Development is not only the purchase of equipment, the construction of facilities, or the publication of a national plan. It is the creation of dependable routines that poor households, older adults, working families, and frontline workers can trust. A small health system develops when it can prevent avoidable illness, respond to sudden shocks, and keep patients connected after the first consultation.
For Caribbean administrators, the difficult question is how to protect quality when scale is limited. A country may not have enough specialists to decentralize every service, yet people still need timely access. This makes referral design, regional agreements, telehealth support, and transport planning central to administration. A service that is clinically available but unreachable for ordinary families remains an incomplete service.
The study also treats social science as a discipline of evidence, not as an opinion layer added to health management. Social science helps administrators read why people behave as they do, how households absorb risk, how trust is formed, and why policies meet resistance. That knowledge can improve appointment design, screening uptake, crisis communication, medicine adherence, and the respectful handling of vulnerable groups.
The region also has strengths that deserve serious attention. Caribbean societies often have close community networks, strong professional commitment, diaspora links, shared public-health institutions, and practical experience with storms, epidemics, and service disruption. Good administration should use those strengths instead of treating smallness only as weakness. The realistic question is how to turn limited scale into sharper coordination: clearer pathways for chronic care, stronger regional purchasing, better community communication, more careful use of data, and service routines that remain dependable when pressure rises.
A Caribbean health administrator has to make decisions with little room for waste. A delayed purchase order may become a medicine gap. A missed outreach visit may become an avoidable hospital admission. A weak referral record may leave a patient with diabetes, hypertension, pregnancy risk, or cancer symptoms moving between offices without anyone owning the next step. These are management problems, but they are also social problems. They show why the subject cannot be left to finance officers, clinicians, or public-health units alone. The strength of the system depends on how well those parts work together around the lives of patients.
A useful Caribbean reform standard must therefore be close to the ground. It should ask whether the mother in a rural community can receive early advice before a pregnancy becomes dangerous; whether the older man with hypertension can refill medicine after a storm; whether a diabetic patient is followed after a missed visit; whether a public-health alert reaches the household in language people trust; and whether a clinic team has enough authority to solve ordinary service breaks before they become emergencies. Those questions give health administration a human measure without turning it into sentiment.
The administrative problem is often hidden in plain sight. Health ministries may know the national rate of diabetes or hypertension, but a clinic manager still needs to know which patients missed review last month, why they missed it, and what can be done before complications appear. A disaster plan may list facilities and emergency contacts, yet an older person who depends on insulin needs a very specific continuity arrangement. Development becomes real when national knowledge is converted into named routines at the level where care is delivered.
This is why small-island health policy should be judged through the patient pathway. The pathway begins before a person enters a clinic and continues after the visit ends. It includes recognition of symptoms, transport, money, family permission, reception, diagnosis, medicine, referral, follow-up, and trust. An administrator who cannot see that full pathway may improve one office while leaving the patient exposed somewhere else.
Chapter 2: Problem Setting and Evidence Base
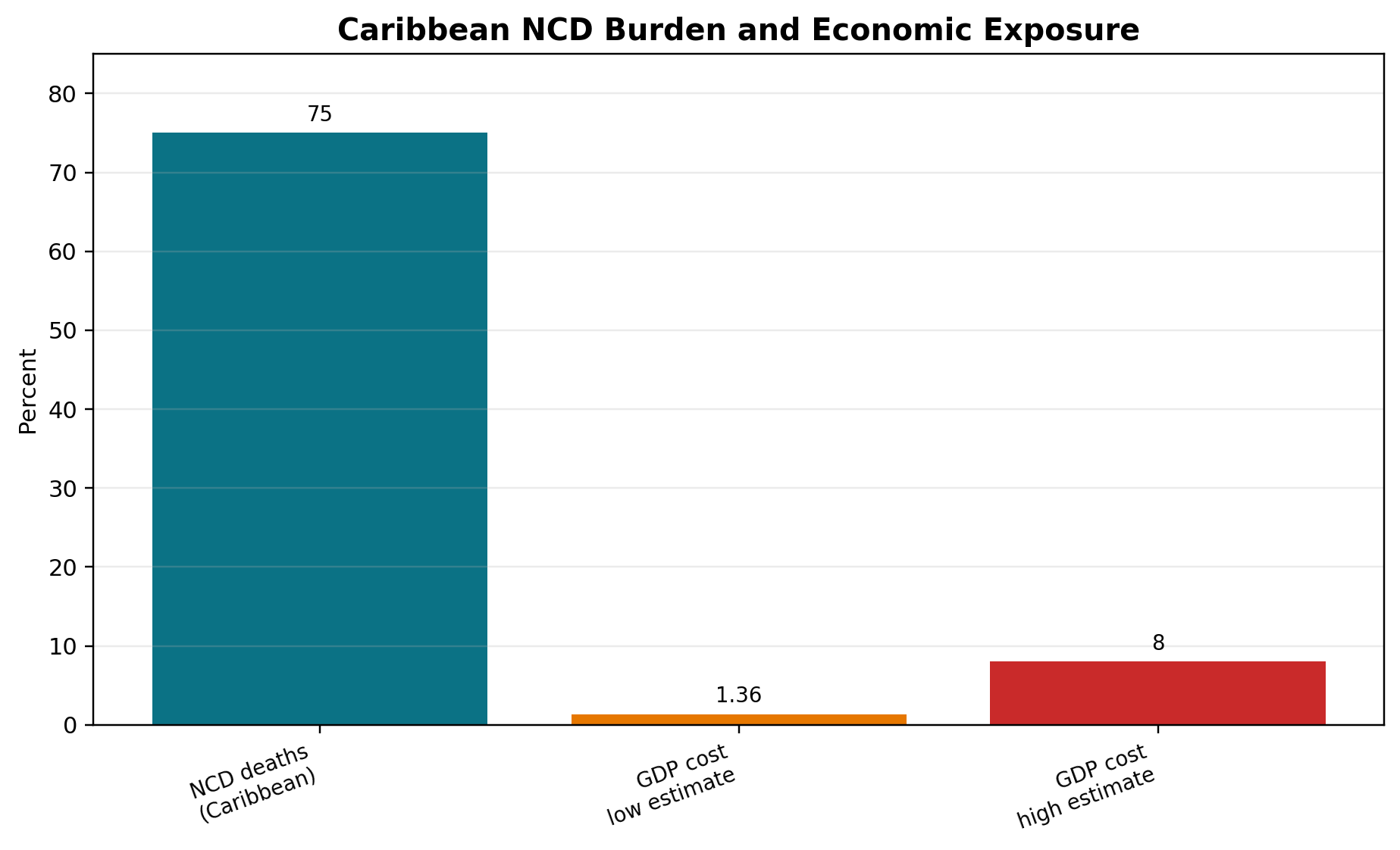
Figure 2. Caribbean NCD burden and economic exposure. Source: World Bank (2024a) and PAHO (2024a). Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Caribbean health systems are often praised for resilience, but resilience should not become a polite word for making do with limited capacity. Small populations can make specialist services expensive. Geographic separation raises referral costs. Tourism-dependent economies may suffer shocks that quickly reduce public revenue. Climate events can damage health facilities and interrupt supply chains. Meanwhile, a growing NCD burden requires long-term continuity, medicine availability, behavior change, community follow-up, and reliable data. Administratively, the system must be acute and chronic, local and regional, clinical and social.
NCDs illustrate the scale of the difficulty. World Bank material on the Caribbean identifies noncommunicable diseases as responsible for roughly 75 percent of deaths in the region and estimates economic costs ranging from 1.36 percent to 8 percent of GDP, before wider indirect family and productivity effects are fully counted (World Bank, 2024a). A figure like that belongs in a finance ministry as much as in a health ministry. Chronic disease drains household income, labor supply, school attendance, caregiving capacity, and national productivity.
The Eastern Caribbean offers a useful case because several states face similar NCD demands while operating with small health workforces and limited specialist capacity. The World Bank’s work on noncommunicable disease care in Dominica, Grenada, and Saint Lucia points toward the need for stronger prevention, earlier detection, primary-care continuity, medicine availability, and patient education (World Bank, 2023). Hospital care remains essential, but it cannot carry the whole burden. Chronic disease is managed through daily routines, not dramatic clinical moments alone.
Table 1. Current Evidence Base for the Caribbean Health Administration study
| Evidence area | Source base | Use in the paper |
| NCD burden | PAHO (2024a); World Bank (2023, 2024a) | Frames chronic disease as both a health and economic development problem. |
| Climate and health | PAHO (2026); WHO (2024) | Links health planning to heat, flooding, vector risk, food security, and facility resilience. |
| Open data | PAHO (2024b); World Bank (2025) | Supports the argument for transparent, ethical, and useful health-information systems. |
| Regional capacity | CARPHA (2025); CARICOM (2022) | Shows why small states need shared surveillance, training, and public-health support. |
| Primary care | WHO (2023); World Bank (2023) | Grounds the recommendation for continuity, screening, medicine reliability, and follow-up. |
Table 1. Current Evidence Base for the Caribbean Health Administration study. Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Climate vulnerability adds another layer. PAHO’s Caribbean climate-health profiles identify the need for stronger risk surveillance, early warning systems, professional training, intersectoral collaboration, and improved access to climate finance for health adaptation (PAHO, 2026). In plain terms, a health ministry cannot stand alone. Disaster management, water authorities, housing, schools, social welfare, local government, meteorological services, and community organizations all become part of health administration once climate events threaten patients, facilities, and public-health routines.
Data remains a central constraint and opportunity. PAHO’s recent open-data work for Caribbean health describes the region as facing resource constraints, a growing NCD burden, and environmental vulnerabilities, while arguing that open data can support transparency, collaboration, and better use of evidence for care and outcomes (PAHO, 2024b). Better data will not solve weak administration by itself, but it can make hidden gaps visible. Clinic attendance, medicine stock-outs, referral delays, screening coverage, waiting times, disaster disruption, and patient follow-up become easier to correct when measured consistently and shared responsibly.
Regional cooperation is not optional in this environment. CARPHA’s Results-Oriented Strategic Plan 2025-2030 presents regional public health as a shared project under the theme of being stronger together (Caribbean Public Health Agency [CARPHA], 2025). A single island may lack scale, but a region can pool knowledge, negotiate better, train jointly, and learn faster. Development, however, still has to reach the household. Social science helps translate regional plans into behavior, trust, and service uptake.
Current evidence also points to a management problem hidden inside the phrase ‘health system strengthening.’ Many governments already know what needs attention: primary care, NCD prevention, medicines, data, emergency readiness, and workforce retention. The harder task is sequencing. Limited budgets force choices. Administrators must decide which reforms produce visible benefit, which reforms protect the poor, and which reforms build capacity for the next crisis. Social science helps by showing where public need and administrative effort are misaligned.
Health expenditure alone cannot answer that question. A small state may spend more per person than a poorer neighbor and still struggle with specialist access or disaster continuity. Another state may run effective community programs despite limited funds because trust, local leadership, and practical coordination are strong. A serious Caribbean study must avoid lazy comparison. Development must be judged through capacity, fairness, reliability, and responsiveness, not spending figures alone.
A further problem is the gap between regional policy language and local implementation. Regional plans often use strong terms, but clinics experience the reality through staffing gaps, study registers, delayed procurement, and uncertain referral routes. This is where administration becomes decisive. The quality of a policy is proven in the ordinary routines of scheduling, supervision, medicine availability, reporting, and follow-up.
The evidence base reveals a double burden of urgency and limited administrative room. Chronic disease needs long-term prevention and care, while climate events require sudden mobilization. These demands compete for money, staff time, and political attention. The better health administration model is one that looks for overlap: community clinics that manage chronic disease can also identify vulnerable patients before storms; strong medicine systems can support daily care and emergency continuity.
Noncommunicable disease control is often discussed through risk factors, but its administrative meaning is continuity. Patients need repeat contact, stable supply, monitoring, education, and adjustment. When any link breaks, complications increase. This is why clinic registers, follow-up lists, medicine forecasting, and referral feedback are not clerical details. They are instruments of prevention.
Climate-health evidence also shows why health planning cannot be locked inside the ministry of health. Heat affects older people and outdoor workers. Flooding affects water quality and transport. Vector-borne disease demands surveillance and environmental action. Food insecurity affects children, diabetes control, and maternal health. A serious administrative response has to bring public works, education, agriculture, social welfare, meteorology, and local government into the health conversation.
Open data has to be handled with care. Transparency can improve accountability, but in small communities data can expose people if privacy is weak. The responsible approach is not to avoid data. It is to build a culture of careful collection, de-identification, ethical use, and practical feedback. Data should help a clinic fix problems, not simply satisfy reporting requirements.
The strongest evidence supports an integrated reading of Caribbean health development. NCD control, climate adaptation, data improvement, workforce planning, and regional cooperation are not separate reforms. They form one administrative challenge: how to make health systems dependable under pressure. That is the frame used throughout the rest of the study.
For that reason, data should be judged by usefulness, not by the number of reports produced. A ministry needs enough information to know where NCD follow-up is failing, which facilities are most exposed to climate disruption, where patients cannot obtain medicines, and which communities do not trust official messages. Open data can improve accountability, but it must be balanced with privacy and local sensitivity. In small societies, careless disclosure can damage trust quickly. The responsible goal is not data display for its own sake; it is timely knowledge that improves decisions.
The evidence base points to one lesson that should guide policy: the main threats do not arrive one at a time. A hurricane can disrupt dialysis, refrigeration, transport, antenatal care, and medicine distribution in the same week. A household affected by diabetes may also face food insecurity, unstable employment, and limited access to safe exercise space. A clinic with a study register may still provide compassionate care, but it will struggle to identify which patients missed appointments after a flood or medicine shortage. Administration has to read these links before the system is tested.
Financing pressure also has to be read with care. Higher spending does not automatically produce stronger access, and lower spending does not always mean weak practice. What matters is the connection between resource decisions and service continuity. A budget that protects medicines, laboratory capacity, community outreach, emergency transport, and staff retention may do more for patients than a visible capital project that does not change the care pathway. Caribbean evidence should therefore be interpreted through the daily movement of patients, goods, workers, and information.
The pressure from noncommunicable disease also changes how success should be measured. A system can report a high number of consultations and still fail to control chronic illness if patients do not receive repeat care, medicine refills, counseling, and timely testing. Chronic care is not a single event. It is a relationship between the patient and the system. That relationship requires steady records, reliable supplies, staff who are not exhausted, and communication that respects the daily life of households.
Climate evidence should be handled with the same discipline. Heat, storms, flooding, and vector risk do not affect every patient equally. People living alone, outdoor workers, pregnant women, persons with disability, people who need dialysis, and households without reliable transport face different forms of danger. Health data should help administrators identify those differences early. The purpose is not to create a more complicated bureaucracy. It is to protect people whose risk is predictable before an emergency makes it visible.
Chapter 3: Why Social Science Belongs Inside Health Administration
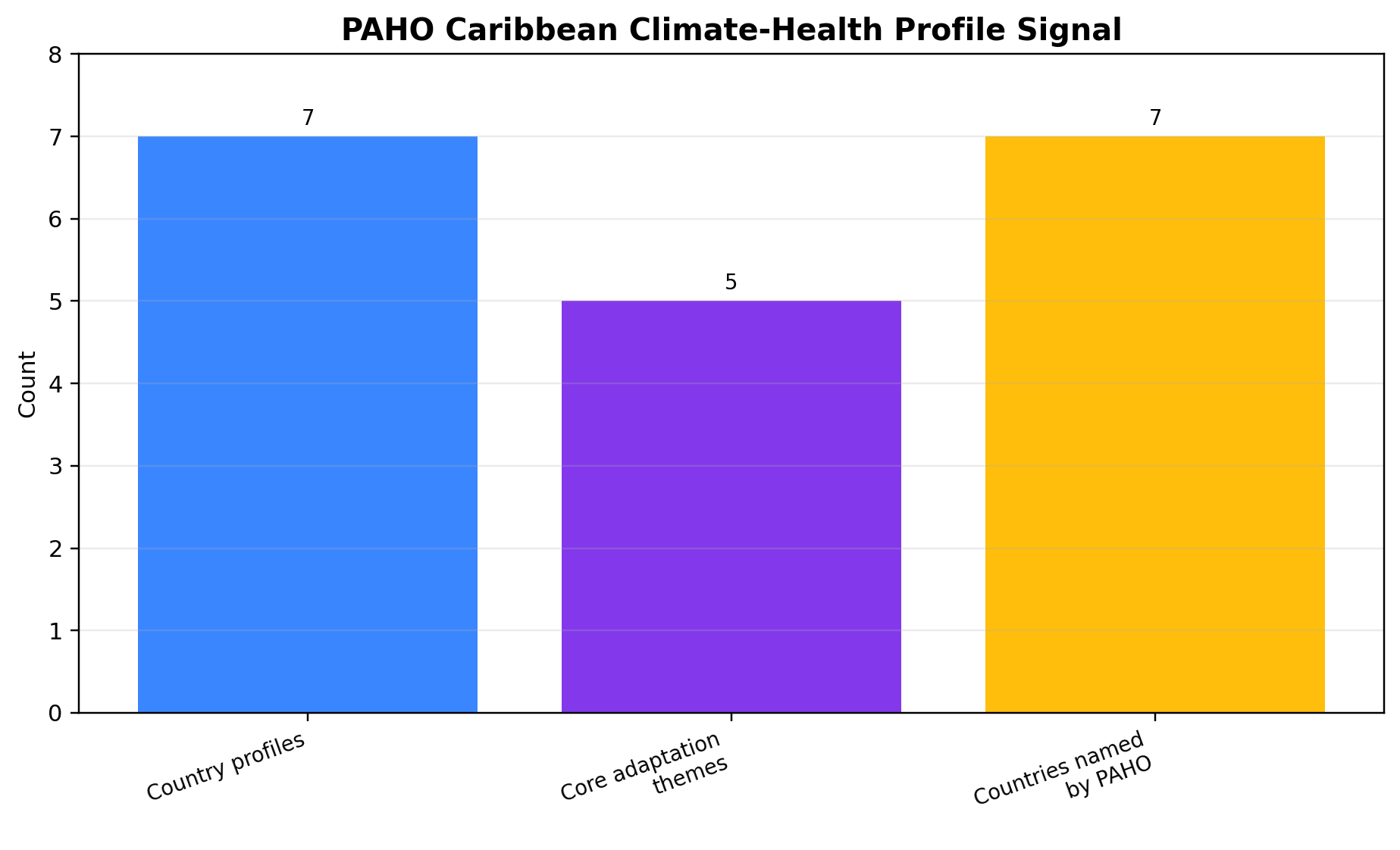
Figure 3. PAHO Caribbean climate-health profile signal. Source: PAHO (2026). Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Health administration often speaks in the language of finance, staffing, infrastructure, and performance targets. Those tools are necessary, but they can become thin if they ignore the social life of care. A patient with uncontrolled diabetes may not simply be nonadherent. Food prices, work schedules, family responsibilities, transport costs, faith, misinformation, depression, clinic waiting time, or distrust of public institutions may shape behavior. Social science gives administrators a disciplined way to interpret these realities without blaming patients for system failures.
For the Caribbean, social science is especially important because communities are closely networked. Family reputation, church life, neighborhood identity, migration histories, and informal caregiving can influence health decisions. Public-health messages about diet, exercise, vaccination, sexual health, mental health, or chronic disease management cannot succeed through posters alone. They have to pass through community authority, cultural memory, household economics, and the credibility of messengers. Administrators who understand these factors can design services that people actually use.
Social science also helps health leaders see inequality. A national average can hide differences between rural districts and urban centers, formal workers and informal workers, older people and young men, citizens and migrants, wealthy families and households that choose between food, transport, and prescriptions. Once those differences are visible, administration becomes more targeted. Primary-care teams can prioritize outreach. Social workers can support households under strain. Community health workers can help maintain contact. Digital tools can reduce friction when designed around access, language, privacy, and trust.
Public trust deserves special attention. During emergencies, people follow advice when institutions have earned credibility before the crisis. Trust grows through honest communication, reliable service, respect at the point of care, and visible follow-up. In small societies, a single poor encounter can circulate quickly. Good administration therefore includes courtesy, complaint handling, patient dignity, and clear communication as much as procurement or accounting. Social science offers methods for listening to community experience and turning it into service improvement.
This does not mean health administration should become sentimental. Social science should strengthen discipline, not replace it. Qualitative evidence, community feedback, behavioral insight, and equity mapping must be used with managerial rigor. If a clinic learns that working adults miss appointments because opening hours conflict with income-generating activity, the administrative response should include scheduling redesign, communication, and follow-up measurement. Listening becomes serious when it changes operations.
The same point applies to NCD prevention. Caribbean diets, food import patterns, advertising, school meals, household budgets, work stress, and public space shape health behavior. Telling people to eat better is weak policy if healthier food is expensive, unsafe neighborhoods discourage exercise, or screening is inconvenient. Social science forces the system to examine the setting in which advice is expected to work. That examination can guide health promotion, taxation, school programs, community partnerships, and primary-care counseling.
Mental health further shows why social science belongs inside administration. Stigma, family silence, religious interpretation, gender expectations, substance use, unemployment, violence, and migration all shape help-seeking. A Caribbean health system that treats mental health only as specialist psychiatry will miss much of the need. Administrators need culturally informed pathways through primary care, schools, workplaces, social welfare, and community organizations. That requires social knowledge as well as clinical knowledge.
Social science also protects against imported reform that looks modern but fits poorly. A digital appointment system can reduce waiting time for some patients while excluding older people or households without stable connectivity. A centralized procurement platform can reduce cost while weakening local responsiveness if not managed carefully. A national dashboard can improve oversight while encouraging shallow reporting if frontline workers are overburdened. Social analysis helps administrators ask who benefits, who is excluded, and how reforms behave in real communities.
The Caribbean therefore needs health administrators who can read budgets and behavior, facilities and families, epidemiology and ethics. That combination should be treated as a core professional competence. It is not an optional humanities addition to technical work. It is part of how a small health system survives pressure while remaining humane.
Social science also helps leaders understand why technically correct policies may fail socially. A dietary campaign can be medically sound and still fall flat if families cannot afford the recommended food. A vaccination campaign can be scientifically valid and still face distrust if communities feel ignored. An appointment system can be efficient on a spreadsheet and still fail workers who cannot leave their jobs during clinic hours.
Behavior should therefore be treated as a design issue. Health administrators should ask what makes the desired behavior easier, safer, cheaper, and more dignified for patients. This question changes the work. It moves a program from telling people what to do toward arranging services so that good decisions are more practical. That shift is essential for NCD care, screening, mental-health support, and emergency preparedness.
Caribbean history also matters. Colonial experience, migration, inequality, and uneven state performance can shape how communities hear official messages. Health communication that ignores history may sound patronizing or distant. A social-science approach does not turn health administration into politics. It helps administrators understand the social memory through which public institutions are judged.
The same logic applies to professional culture. Doctors, nurses, pharmacists, community health workers, clerks, ambulance teams, and social workers all carry different habits and pressures. Administrative reform fails when it assumes staff will change behavior because a policy says so. Social science helps leaders understand incentives, workload, identity, fear, morale, and the informal routines that drive practice.
A second professional implication is the need for humility in reform design. Good models should travel as principles, not as copies. Administrators and practitioners must ask whether the financing, workforce, law, infrastructure, and culture of a setting can carry a proposed intervention. Where capacity is limited, sequencing matters. The better question is not what sounds impressive in a strategy document, but what can be delivered reliably and improved over time.
Placed inside administration, social science also protects policy from blaming patients too quickly. Missed appointments, late presentation, poor medicine adherence, and weak participation in prevention programs often reflect barriers that administrators can reduce. Clinic hours, queue systems, payment rules, referral distance, language, gender dynamics, disability access, and previous mistreatment all affect behavior. A health system that studies those realities is not being sentimental. It is trying to manage risk more accurately and spend public resources where they will change outcomes.
Social science helps explain the gap between a policy that is correct and a service that people actually use. Patients may avoid screening because they fear cost, shame, bad news, transport loss, or disrespect. Families may rely on informal advice before seeking care. Workers may resist new reporting tools because they see them as extra paperwork rather than support. Community leaders may influence whether a health warning is believed. None of these issues can be fixed by a budget line alone. They require listening, design, communication, and feedback.
Administrative decisions also create social meaning. When a ministry closes a local service without explaining the alternative, communities may read the decision as abandonment. When health workers speak down to patients, people may delay care the next time symptoms appear. When data is collected but no visible action follows, trust declines. Social science gives leaders a way to notice these effects early. It helps them understand why formal authority is not the same as public confidence and why reform must be communicated through relationships as well as documents.
Public-health messages often fail when they are technically accurate but socially weak. A warning about diet may be useless where healthier food is expensive. A message about screening may not reach men who avoid clinics until pain becomes severe. Advice about mosquito control may not work where waste collection, drainage, and housing conditions are poor. Social science forces health administration to connect advice with the conditions in which people are being asked to act.
It also improves leadership inside institutions. Staff morale, professional identity, informal workplace culture, and trust in management affect whether reforms are carried out honestly or treated as another temporary instruction. A new reporting tool may be rejected because it adds work without solving a real problem. A referral policy may be ignored because the receiving service is known to be slow. Administrators need social evidence inside the workforce as much as they need it in the community.
Chapter 4: Case Evidence from the Caribbean
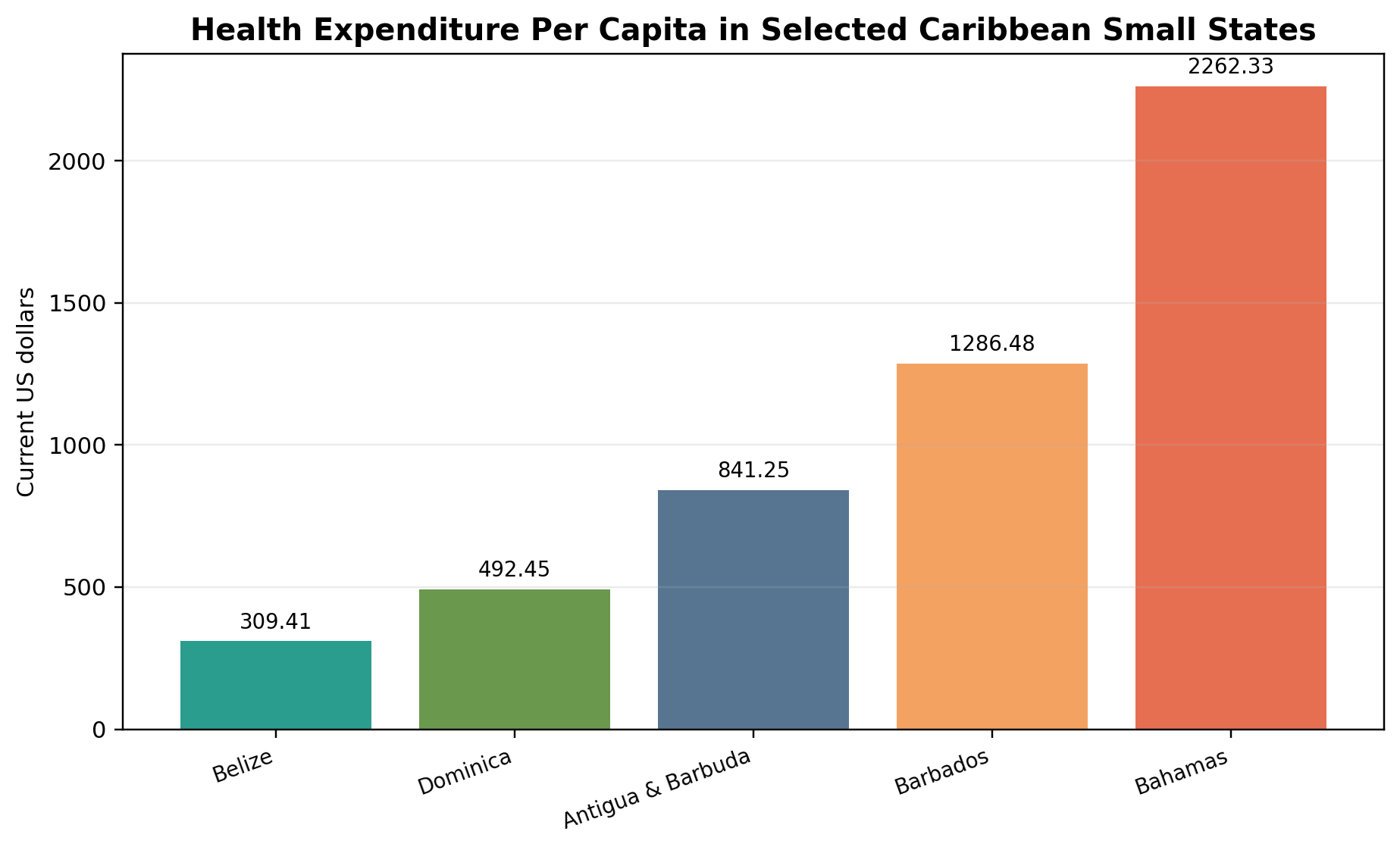
Figure 4. Health expenditure per capita in selected Caribbean small states. Source: World Bank World Development Indicators (2025). Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
The first case area is noncommunicable disease care in the Eastern Caribbean. Dominica, Grenada, and Saint Lucia have been examined in recent World Bank work because NCDs create long-term service demands that cannot be solved by hospital treatment alone (World Bank, 2023). These countries show why primary care must become a center of health administration rather than a low-status entry point. Screening, medicine continuity, patient education, referral, and follow-up require routine reliability. A missed prescription can become a stroke. A missed foot check can become an amputation. A missed appointment can become a crisis admission.
Social science sharpens the lesson. Diabetes and hypertension are not managed only by clinical instruction. Diet depends on income, food availability, family habits, work schedules, and cultural meaning. Exercise depends on safety, time, transport, and public space. Medication adherence depends on cost, side effects, health literacy, trust, and the relationship with the clinic. Administrators who treat NCD control as a supply problem alone will keep missing these barriers. The Eastern Caribbean case supports integrated planning: primary care teams, community education, medicine supply, social support, and data feedback.
The second case area is Trinidad and Tobago’s public-health planning and demographic change. PAHO’s 2024 country profile shows an older population and the need to adapt services as age-related needs grow (PAHO, 2024c). Aging changes health administration. More people require chronic-disease management, rehabilitation, home support, mobility planning, and caregiver assistance. The system has to plan beyond hospitals because older adults experience health through transport, housing, family care, income, medicine access, and social connection.
Aging also raises workforce questions. Health workers may leave, retire, or seek better opportunities abroad. The remaining workforce must carry heavier chronic-care loads. Administrators cannot fix this through recruitment alone. They need retention strategies, training routes, supervision, respectful working conditions, and smarter task distribution. Social science helps explain why professionals stay, why they leave, and what forms of recognition matter in small labor markets. It also helps leaders understand the family pressures that health workers carry outside the workplace.
The third case area is open data. PAHO’s Caribbean health data work highlights a region trying to improve evidence use while facing resource constraints (PAHO, 2024b). Good data can reveal where services fail: who misses follow-up, where medicine stock-outs occur, which communities are under-screened, and which clinics face rising waiting times. Data should not be treated as a bureaucratic burden. When used well, it becomes a management instrument for fairness.
Data also creates ethical duties. Small populations can make individuals easier to identify, especially in sensitive areas such as HIV, mental health, sexual violence, disability, and migration status. Administrators must balance transparency with privacy. Social science can support this balance by asking how communities perceive data use, whether reporting builds trust, and how information can be shared without exposing people to harm. In a region of small communities, data governance is not a technical afterthought. It is a public-trust issue.
The fourth case area is climate-health adaptation. The 2026 Caribbean climate-health profiles show that countries are already facing hazards linked to heat, flooding, sea-level rise, vector-borne disease, food insecurity, and infrastructure stress (PAHO, 2026). Health administration must prepare facilities, staff, medicine supply, emergency communication, and community follow-up before events occur. Climate readiness also requires attention to mental health, displacement, older adults, persons with disabilities, and households without savings.
Climate risk reinforces the value of regional cooperation. One island’s laboratory capacity, technical training, or emergency experience can benefit another. CARPHA’s strategic plan recognizes the regional nature of public health threats and the need for shared capacity (CARPHA, 2025). Yet regional strength cannot erase local responsibility. Each country still needs working referral lists, emergency stock rules, patient communication, and clinic-level preparedness. A regional plan becomes real only when facilities know what to do on a difficult morning.
The final case area is community trust. Caribbean health systems depend on formal ministries and informal networks at the same time. Churches, schools, local leaders, youth groups, diaspora ties, and neighborhood associations can strengthen health promotion when they are treated as partners rather than audiences. Trust is not built by occasional consultation. It is built when the system returns with answers, admits limits, and makes visible improvements. Administrators who treat communities as passive recipients weaken the very cooperation they need.
The case evidence also cautions against treating each country example as a showcase. The purpose of case study work is not admiration. It is disciplined learning. Each case reveals a tension: how to manage chronic disease without enough specialist capacity, how to use data without harming privacy, how to prepare for climate events without unlimited funds, and how to build trust when public patience is limited.
The Eastern Caribbean NCD case is especially important because it shows the weakness of hospital-centered thinking. Hospitals are necessary, but chronic disease develops and worsens in daily life. A patient does not become hypertensive in the hospital. Poor diet, stress, medication gaps, family history, work pressure, and missed screening often precede the crisis. Administration must therefore move upstream without abandoning acute care.
Trinidad and Tobago’s demographic profile offers another lesson. Aging does not only increase clinical need; it changes the social organization of care. Families may be smaller, caregivers may live abroad, and older adults may need transport or home support. Health administration has to plan for these realities before they arrive as overcrowded clinics and avoidable admissions.
The open-data case should be read as a management discipline. A dashboard that does not change decisions is decoration. A report that does not reach clinic managers is weak oversight. Data becomes useful when it is tied to responsibility: who sees the gap, who has authority to act, who receives feedback, and how the public knows improvement occurred.
Climate-health case evidence confirms that the future health administrator must be comfortable with uncertainty. Storms, heat, floods, and disease patterns do not wait for perfect budgets. The practical question is which basic systems can keep working when conditions deteriorate. Facilities, staff rosters, supply chains, patient lists, and communication channels must be designed with interruption in mind.
One useful lesson is that small systems can move faster when roles are clear. Regional bodies can support surveillance, procurement, laboratory capacity, training, and emergency guidance, while national services remain responsible for the patient experience. Community clinics can identify risk early, but they need referral routes that work. Ministries can publish data, but facility managers must be able to act on it. Caribbean health development will gain more from tightening these links than from creating another layer of policy language.
The case material shows why regional learning matters. Eastern Caribbean NCD care, Trinidad and Tobago’s planning context, climate-health profiles, and regional open-data work are not identical examples, but they expose the same administrative pressure: chronic disease requires continuity, climate risk requires preparedness, and public trust requires communication that people recognize as credible. A good case-study approach should not force these examples into a single template. It should read them as practical evidence of where systems break and where coordination can improve.
Trinidad and Tobago also illustrates the need to join planning with follow-through. A relatively stronger resource base does not remove the need for clear priorities, community-level prevention, risk communication, and reliable chronic-care pathways. Larger Caribbean states may have more institutional depth than smaller neighbors, but they still face public expectations, social inequality, professional pressure, and climate exposure. The lesson is not that one country should become the model for all others. The lesson is that every territory must translate policy capacity into visible care discipline.
The Eastern Caribbean examples are especially useful because they show how chronic-care weakness can travel across small systems. A shortage in one service point, a delayed laboratory result, a weak referral form, or a missing medicine can affect a patient for months. The lesson is not simply that more money is needed, although funding matters. The deeper lesson is that continuity has to be designed. Patients with long-term conditions need a system that remembers them, not a series of disconnected contacts.
Regional open-data work adds another practical lesson. Public information can strengthen accountability only when it is translated into decisions that workers and communities can recognize. A dashboard that shows risk by disease, age, location, or facility can help managers act earlier. Yet if data is published without explanation, privacy protection, or local follow-up, it may produce suspicion rather than trust. Caribbean data reform must therefore be both technically competent and socially careful.
Caribbean case evidence should also be read with humility. Public sources can show disease burden, financing pressure, climate exposure, and system priorities, but they cannot capture every local decision made by a nurse, pharmacist, community worker, or patient. That limitation does not weaken the analysis; it keeps the analysis honest. The purpose is to draw careful administrative lessons from available evidence and to identify where future local inquiry would strengthen policy. Good health administration uses public data, but it also knows when the numbers must be checked against service experience.
Chapter 5: Development Priorities for Caribbean Health Administration
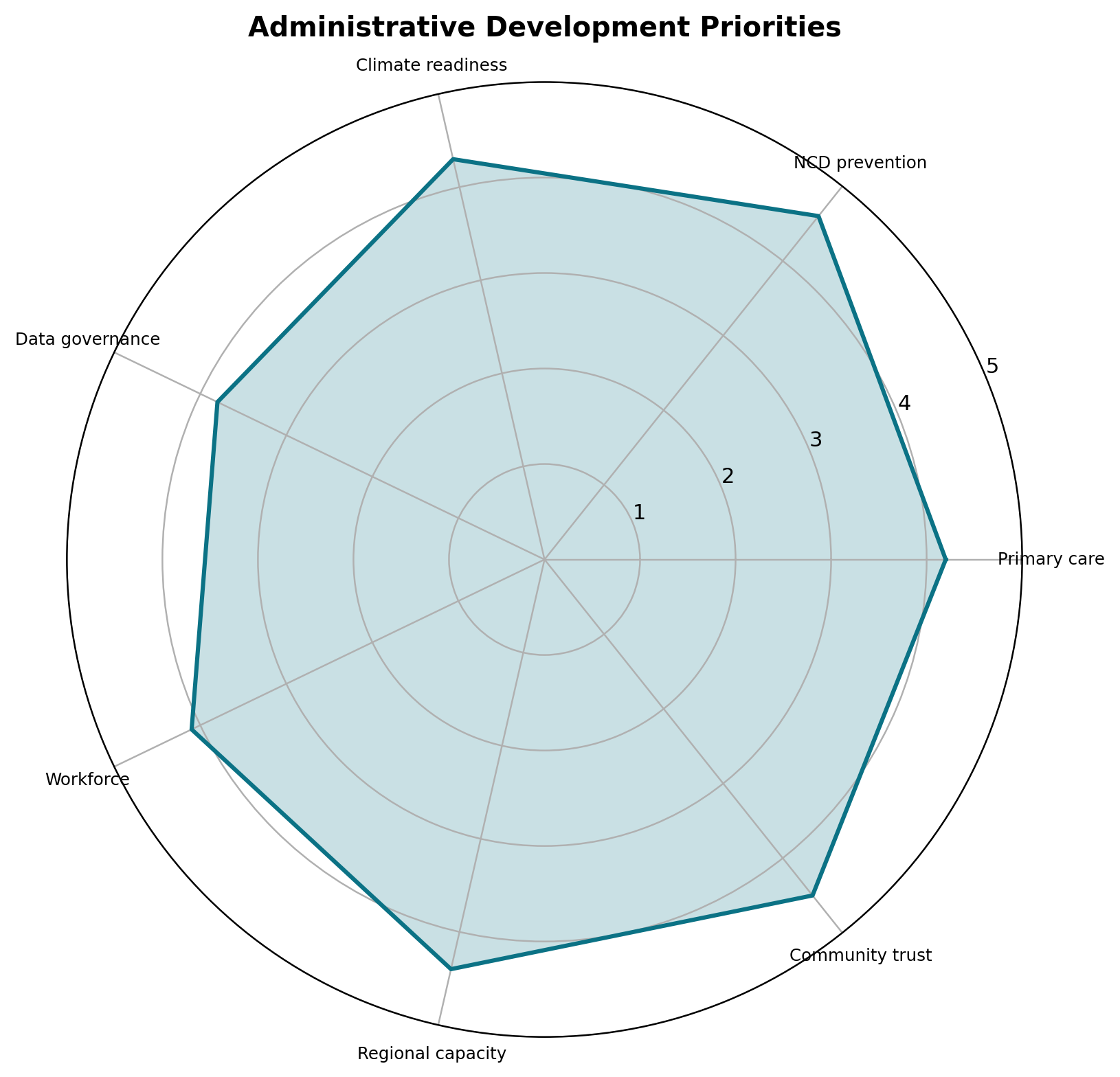
Figure 5. Administrative development priorities for Caribbean health systems. Source: Author analytical framework. Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Caribbean health reform keeps returning to the hospital because the hospital is visible. It has buildings, machines, specialists, ceremonies, budgets, and political value. The clinic has less prestige, but it is where many expensive failures begin. A patient misses blood-pressure medication. A diabetic wound is not checked. A mother misses review. A referral goes nowhere. No one follows up. Months later, the hospital receives what the clinic should have caught.
That is the real administrative test. Does the clinic know its patients? Are the medicines there? Is the register current? Did anyone call the patient who missed review? Did the referral come back with an answer? Can the nurse explain treatment in a way the family understands? These are not soft questions. They decide whether chronic illness stays manageable or becomes stroke, kidney failure, amputation, maternal crisis, or another preventable admission.
Primary care in the Caribbean cannot remain thin and underpowered. It needs authority, staff, medicine, records, transport links, and enough trust to keep people in care. A clinic without a working register is guessing. A pharmacy without stock control is gambling with patients. A referral system without feedback is not a system. It is a handoff into uncertainty.
Noncommunicable disease makes the weakness impossible to hide. The World Bank’s estimate that NCDs account for about 75 percent of Caribbean deaths should disturb any health plan that still treats chronic illness as a side program (World Bank, 2024a). Diabetes, hypertension, heart disease, kidney disease, and stroke risk sit inside household income, food cost, transport, work pressure, fear, and trust. A campaign can raise awareness. It cannot replace steady care.
Chronic care is built from habits that look ordinary until they fail. The register is updated. The medicine arrives. The patient is recalled. The wound is checked. The blood pressure is reviewed. The referral is traced. The clinic manager looks at the data and corrects what is slipping. Where those habits are absent, the damage accumulates quietly. The bill comes later, in disability, hospital cost, lost wages, and grief.
Climate risk now punishes weak routines faster. A flood closes a road. A generator fails. Medicine storage is compromised. Staff cannot travel. A patient on insulin, dialysis, antiretroviral therapy, psychiatric medication, or maternal care is cut off. Preparedness is not the binder in the ministry office. It is the patient list, the stock rule, the backup power, the protected storage, the emergency route, and the message that reaches people before panic does.
Staff loss cuts just as deeply. In a small island system, one experienced nurse, pharmacist, laboratory officer, public-health worker, or doctor can hold together more than the job title suggests. That person carries patient memory, local judgment, informal knowledge, and the trust of people who may not trust the institution itself. When such workers leave, the loss is not a line on a staffing table. It is a service made weaker. Pay matters, but so do workload, safety, supervision, promotion, training, and respect.
Regional cooperation is useful only when it performs. Shared procurement, laboratory support, surveillance, training, and emergency coordination can help small states avoid paying alone for every capacity they need. CARPHA’s role matters because health threats and supply shocks cross borders (CARPHA, 2025). But cooperation that moves slowly, hides its rules, or fails under pressure will not hold trust. Countries need prices they can defend, delivery they can rely on, and arrangements that work when demand rises.
Poverty cannot be treated as an outside issue. A patient can receive the right diagnosis and still lose the treatment battle because transport is too costly, food is uncertain, wages are lost, or caregiving takes over the day. When that happens, the clinic may record “noncompliance,” but the real story is harder. Care failed to meet the conditions of the patient’s life. Health services need working links to welfare support, disability services, food assistance, child protection, legal aid, and trusted community organizations.
Digital health needs the same realism. Records, reminders, telehealth, dashboards, and surveillance platforms can help a clinic find patients before they disappear. They can also leave out older adults, rural households, low-literacy patients, migrants without stable papers, people without smartphones, and families with no privacy at home. A useful digital tool helps staff act earlier and protects the patient. A bad one turns care into another reporting exercise.
Accountability belongs at the counter, the clinic room, the pharmacy, and the referral desk. Patients know when medicines are missing. They know when staff speak down to them. They know when a referral leads nowhere. They know when nobody calls after a missed appointment. Health workers know whether honesty is safe. Communities know whether consultation brings correction or just another attendance sheet.
Caribbean health reform has to prove itself there. Not in launch language. Not in a longer strategy. In the clinic that remembers the patient, the pharmacy that has the medicine, the worker who stays, the data that changes a decision, and the community that sees the system keep its word.
Development priorities need sequence. A ministry that tries to launch every reform at once may exhaust staff and lose credibility. A better approach begins with conditions that create the greatest burden and services that patients use most often. Primary care, medicines, referral feedback, and chronic-care follow-up should be early priorities because they produce visible benefits and reduce preventable pressure on hospitals.
Another priority is the redesign of managerial attention. Senior leaders often focus on budgets, procurement, and national targets, while frontline managers struggle with waiting rooms, staff shortages, and missing supplies. A stronger system connects these levels. Data from clinics should inform national decisions, and national decisions should solve real clinic problems. The middle layer of management is therefore critical.
Workforce retention should be treated as a quality issue. When skilled workers leave, patients lose relationships and systems lose memory. Replacement hiring cannot fully replace the local knowledge of experienced staff. Caribbean administrations need career pathways, mentoring, regional training, workload review, and respectful leadership. Retention is often cheaper than repeated recruitment.
Regional procurement and shared capacity require trust among governments. States must believe that pooled systems will be fair, timely, and transparent. Without that trust, every country will retreat into smaller and more expensive solutions. Governance design is therefore as important as technical design. Regional institutions should publish clear rules, performance information, and dispute mechanisms.
Digital health deserves steady ambition rather than fashionable enthusiasm. The best digital tools reduce friction for patients and staff. They remind patients, protect records, support medicine planning, and allow managers to see gaps early. The worst tools create double reporting, privacy fear, and exclusion. Caribbean administrations should judge technology by service effect, not by novelty.
A second professional implication is the need for humility in reform design. Good models should travel as principles, not as copies. Administrators and practitioners must ask whether the financing, workforce, law, infrastructure, and culture of a setting can carry a proposed intervention. Where capacity is limited, sequencing matters. The better question is not what sounds impressive in a strategy document, but what can be delivered reliably and improved over time.
The second priority is resilience that reaches beyond buildings. A stronger facility matters, but a climate-ready system also needs emergency patient lists, protected medicine storage, heat plans for older people and outdoor workers, transport arrangements, staff backup, communication channels, and coordination with water, housing, education, and local government. Disaster readiness must be written into routine administration before the storm arrives. Once a crisis starts, weak routines become expensive and dangerous.
The first priority is continuity of care. Chronic disease management depends on repeat contact, reliable medicines, laboratory access, referral completion, counseling, and family support. A patient who receives advice once and then disappears from the system is not being managed. Administrators should therefore ask practical questions: Which patients missed follow-up? Which facilities reported medicine gaps? Which referrals were not completed? Which communities show low screening uptake? Those questions move performance measurement closer to the real work of prevention and care.
Workforce planning deserves the same practical treatment. Caribbean countries cannot build stable services if nurses, doctors, pharmacists, public-health officers, and allied professionals feel replaceable, unsupported, or trapped in weak career pathways. Retention is not only a personnel matter. It affects waiting time, continuity, patient trust, supervision quality, and institutional memory. Administrators should therefore treat workforce data as development evidence: who is leaving, why they leave, what roles are hardest to fill, and which support measures make service more stable.
Procurement belongs near the center of the development agenda. Imported medicines, equipment, spare parts, and diagnostic supplies expose small states to price changes, shipping delays, and global competition. A weak procurement system does not fail quietly. It appears as cancelled appointments, untreated symptoms, pressure on nurses, angry patients, and avoidable referrals. Regional purchasing and shared stock intelligence can reduce some of that risk, but the national system still needs disciplined forecasting, storage, reporting, and accountability.
Digital health should be approached with the same caution. Electronic records and dashboards can strengthen continuity, but they will not fix poor workflow by themselves. A digital tool that is too slow, too complex, or disconnected from daily practice becomes another burden. The better route is to begin with the decisions that staff must make: who needs follow-up, where supplies are running low, which referrals are overdue, and which households face high climate or social risk. Technology should serve those decisions.
Chapter 6: Social Development, Equity, and Community Trust
Health administration and social development meet at the household. A clinic can diagnose hypertension, but the household decides whether medicine is bought, stored, taken, and continued. A public-health campaign can encourage screening, but the household decides whether fear, transport cost, or stigma wins. A disaster plan can list evacuation centers, but families decide whether older relatives, disabled persons, and children can move safely. Social development is therefore not outside health. It is one of the conditions that makes health care work.
Equity has to be operational, not decorative. A health system can claim universal access while poor households face indirect costs that quietly exclude them. It can offer screening while rural communities lack transport. It can publish digital information while older people or poorer households cannot use it. Equity means the system identifies these barriers and redesigns service around them. It also means measuring who is left behind rather than assuming national coverage figures tell the whole story.
Community trust is a form of health infrastructure. It is less visible than a hospital building, but it can decide whether people accept vaccination, disclose symptoms, attend clinics, or follow emergency guidance. Trust is damaged by disrespect, long waits, missing medicines, confusing instructions, and officials who appear only during crisis. Trust is built through consistency. When a clinic is reliable, when staff explain care, when complaints are handled, and when referrals are followed up, people begin to believe the system sees them.
Table 2. Caribbean Administrative Priorities and Social Science Contribution
| Priority | Administrative task | Social science contribution |
| NCD control | Screening, registries, medicine supply, recall, referral feedback | Explains adherence, diet, stigma, family support, and health literacy. |
| Climate readiness | Facility continuity, early warning, emergency stock, vulnerable-patient registers | Maps risk perception, displacement, trust, caregiving, and household vulnerability. |
| Workforce retention | Training, supervision, career pathways, workload review | Assesses motivation, migration intent, burnout, and professional dignity. |
| Digital health | Records, dashboards, telehealth, surveillance, privacy rules | Protects equity, access, trust, privacy, and meaningful interpretation. |
| Community trust | Complaint handling, respectful communication, feedback loops | Turns patient experience and community knowledge into service repair. |
Table 2. Caribbean Administrative Priorities and Social Science Contribution. Copyright © June 2026 Favour I. Onyebuchi / NYCAR.
Social science gives administrators practical tools for trust building. Patient-experience interviews, community mapping, focus groups, complaint analysis, participatory planning, and behavioral insight can reveal why services are not used. Those tools should not become symbolic exercises. If communities explain that waiting time, transport, or staff conduct is discouraging attendance, the system should respond with scheduling change, transport links, staff support, or communication reform. Listening without action weakens trust.
Gender deserves specific attention. Women often carry caregiving responsibilities, maternal-health risk, unpaid labor, and responsibility for children’s appointments. Men may avoid care because of work pressure, pride, fear, or social expectation. Young people may avoid sexual and mental-health services because confidentiality feels unsafe. Migrants may avoid services because of documentation concerns. Social development requires health systems to understand these patterns and design care with them in mind.
Poverty also changes the meaning of health advice. A doctor may recommend diet change, but imported healthy foods may be expensive. A nurse may advise follow-up, but the patient may lose a day’s income to attend. A mental-health worker may recommend rest, but a household may survive on informal work. Administrators should not turn poverty into a moral failing. They should design services that reduce friction: longer prescription intervals where safe, community refills, appointment reminders, outreach, and coordination with welfare systems.
The diaspora is another Caribbean reality. Families are often spread across countries, and remittances can support care. Digital communication may allow relatives abroad to help with appointments, payment, or information. At the same time, migration can reduce local caregiving and drain professional capacity. Health administration should understand diaspora ties as part of the care environment. They are not a replacement for public systems, but they shape household resilience.
Children and older people are especially affected when health and social services fail to connect. A child with asthma, malnutrition, disability, or trauma may need school support, family assessment, safe housing, and nutrition assistance. An older adult with diabetes may need transport, medicine management, social contact, and caregiver support. A clinic that treats the disease but ignores the living situation may record a completed episode while the patient remains unsafe. Social development thinking prevents that kind of false success.
Community trust also protects reform from political fatigue. Caribbean countries have seen many strategies, projects, and donor-supported plans. People judge new promises by old experience. A careful administrator should therefore avoid exaggerated reform language and focus on visible service improvement. The most persuasive reform is the one patients can feel without reading a policy document.
Equity also requires administrators to look at informal costs. A service may be free at the point of care but expensive in practice if transport, food, childcare, or lost wages are high. These costs are easy for institutions to overlook because they do not appear in the health budget. Patients carry them silently, and missed care becomes the evidence of that burden.
Community trust should be built before emergencies. A hurricane warning, disease alert, or vaccination campaign will be received through the memory of everyday service. If people routinely experience disrespect or unreliability, emergency communication will face suspicion. If clinics are known for fairness and clear explanation, public-health advice has stronger ground.
The social development view also helps explain why health and education are connected. Schools can support screening, nutrition, mental-health awareness, vaccination, and health literacy. Children often carry health messages home. At the same time, illness can push children out of school or reduce performance. Health administration that ignores education loses a major channel for prevention and early support.
Gender-sensitive planning should not be reduced to maternal health alone. Women may need maternal care, but they also need chronic-disease care, mental-health support, protection from violence, and recognition of unpaid caregiving labor. Men may need service designs that reduce shame and fit work realities. Young people need confidentiality and respect. Social science helps make these differences administratively visible.
The point is not to create a separate social agenda beside health. The point is to make health service design honest about the conditions that shape use. A patient’s ability to follow advice is affected by the household, the workplace, the road, the clinic, the price of food, and the behavior of staff. Equity begins when administration accepts that full picture.
Equity also requires administrators to see indirect costs. A service may be officially free and still be difficult to use because transport is expensive, work time is lost, child care is unavailable, or patients fear stigma. Older people, persons with disability, migrants, low-income families, and residents of remote communities often feel these barriers more sharply. Social development in health administration means designing services so that these groups are not treated as afterthoughts. The test is whether the pathway works for people with the least room to absorb failure.
Trust is built in small administrative moments. A patient notices whether the clinic opens on time, whether the nurse explains clearly, whether the medicine is available, whether a complaint is treated with respect, and whether the system follows up after referral. Communities also remember how institutions behaved during crisis. That memory affects later vaccination campaigns, NCD screening, mental-health outreach, and climate warnings. Trust therefore belongs in management review, not only in public speeches. It should be studied through patient experience, missed visits, complaints, outreach participation, and referral outcomes.
Communication should also be treated as an administrative function. It is not enough to issue warnings or publish advice after risk appears. The system needs trusted messengers before crisis, including nurses, community workers, teachers, religious leaders, local councils, disability advocates, youth groups, and media partners. These relationships cannot be created overnight. They are built through routine contact, respect, and honesty. In the Caribbean, where communities are often close and memory is long, credibility can become one of the strongest public-health assets.
Equity is also about how power is experienced. A patient may feel unable to ask questions because the clinic culture is intimidating. A migrant may avoid services because of fear or documentation uncertainty. A person with mental distress may delay care because stigma is stronger than the symptom. A disability advocate may see access problems that the facility has normalized. Health administrators who listen to these experiences can correct service failures that are not visible in budget tables.
Community trust should not be confused with public approval. People may praise a health worker and still avoid the system when they expect delay or disrespect. They may trust a local nurse more than a national campaign. They may listen to a pastor, teacher, radio host, or community elder before a ministry spokesperson. Caribbean systems should work with that reality. The goal is not to surrender professional standards to rumor. It is to carry reliable health information through channels that people actually use.
Chapter 7: Implementation Agenda
Caribbean health reform cannot begin with another polished plan. The region has enough plans. What is often missing is a clear view of the patient’s actual journey: where care begins, where delay enters, where referral breaks, where medicine supply fails, where records stop being useful, and where the patient quietly disappears. A ministry that cannot describe that journey for diabetes, hypertension, maternal care, child health, cancer screening, mental health, emergency care, and climate disruption is managing too much from above.
The first useful exercise is therefore simple: follow the patient. Not in theory, but through the real service. A woman with a high-risk pregnancy enters one clinic, waits for review, receives a referral, travels to another facility, returns home, misses one appointment, and may or may not be traced. A man with uncontrolled hypertension receives medicine for one month, returns when the pharmacy has none, then comes back later with a stroke. A diabetic patient is screened, referred, delayed, and seen again only when a wound has worsened. These are not unusual stories. They are the places where administration either protects life or wastes it.
The best evidence for reform often sits with the people closest to the service. Clinic nurses know which patients miss review because transport is costly. Pharmacists know which medicines fail repeatedly. Ambulance teams know which roads become useless after heavy rain. Community health workers know which families are embarrassed to ask for help. Patients know which desk sends them away without an answer. None of this requires expensive research to discover. It requires leadership willing to listen without turning every conversation into ceremony.
A service map has value only when it leads to correction. If it shows that referrals disappear, someone must own that failure. If medicine stock fails in the same clinic every quarter, the reason must be traced. If cancer screening reaches the same easy communities while poorer settlements remain outside the net, outreach has to change. If mental-health patients are lost after the first appointment, the follow-up routine has to be rebuilt. Mapping without repair is another way of decorating failure.
Primary care is where much of this repair has to happen. A clinic managing chronic disease cannot work with stale registers, loose referrals, uncertain medicine supply, and follow-up that depends on staff memory. It needs records that tell the truth, stock information that reaches the right office early, patient education that people understand, and a recall routine that does not wait for crisis. A patient with diabetes, hypertension, asthma, HIV, depression, pregnancy risk, or disability should not need luck to remain inside the health system.
Continuity is the treatment in chronic care. The tablet matters, but so does the refill. The blood-pressure check matters, but so does the next review. A referral matters only if the patient reaches the next service and the clinic receives feedback. A foot check matters because it may prevent infection, surgery, and lifelong disability. The ordinary parts of care carry the weight. Caribbean health administration has to become serious about these ordinary parts because hospitals are already carrying the cost of neglect.
Social risk cannot be treated as background noise. A patient may understand the diagnosis and still fail treatment because there is no transport money, no stable food supply, no safe housing, no caregiver relief, or no way to miss work without losing wages. Some patients live with violence, mental distress, disability, or fear of being exposed. A clinic that does not see those pressures will keep calling them noncompliance.
Screening for social risk has to be modest, careful, and useful. Staff should not collect sensitive information because a form demands it. They should ask only what can be protected and acted on. Where hardship is found, there must be a route to help: welfare support, disability services, food assistance, child protection, legal aid, mental-health care, emergency protection, or a trusted community organization. Asking patients to disclose hardship and then offering nothing damages trust.
Climate continuity belongs inside daily management, not in a binder waiting for storm season. Every facility ought to know which patients cannot safely lose contact with care. Dialysis patients. Insulin-dependent diabetics. Pregnant women near term. People on antiretroviral therapy. Patients taking psychiatric medication. Older adults living alone. Children with complex conditions. Persons with disability. These names should be known before the flood, heat event, water failure, or power cut arrives.
A climate plan proves itself under pressure. Can the clinic reach the patient? Can the pharmacy protect medicines? Can staff communicate if the normal channel fails? Is there backup power? Is water available? Does the district team know the emergency route? Who has authority when the usual chain is broken? A plan that cannot answer these questions is not readiness. It is paperwork.
Workforce support also has to become more honest. Caribbean ministries often speak about recruitment while saying less about why trained people leave. The harder questions are local and uncomfortable. Which facility is overloaded? Which supervisor is driving staff away? Which workers have no advancement route? Which training promises never reach the workplace? Which clinic is being held together by one tired nurse everyone depends on? Those questions cannot be answered in a public meeting where staff fear punishment for speaking plainly.
Retention is not only salary, although salary matters. It is workload, safety, supervision, training, mentorship, promotion, housing pressures, family life, and professional respect. A pharmacist, public-health inspector, nurse, laboratory officer, doctor, or community health worker carries knowledge that a vacancy report cannot show. When such a person leaves, the service loses memory, judgment, patient trust, and informal problem-solving. Small systems cannot afford to learn this lesson repeatedly.
Regional learning has to become more useful and less ceremonial. CARPHA, PAHO, CARICOM, universities, and national ministries can help with short courses, procurement forums, data standards, emergency drills, peer review, and technical exchange. The value is not in the meeting itself. The value is whether a clinic manager, pharmacist, district nurse, public-health officer, emergency team, or laboratory lead returns with a tool that changes work.
Shared capacity is necessary where national scale is too small. Procurement, laboratory networks, specialist consultation, emergency guidance, professional training, surveillance, and analytics cannot all be carried efficiently by each country acting alone. Regional support, however, must reach the service level. A regional agreement that does not improve the clinic, pharmacy, ambulance, public-health unit, or home visit will remain distant from the patient.
Data governance deserves stricter handling in small societies. Open data and internal dashboards can improve management, but Caribbean populations are close enough for privacy to be fragile. HIV status, mental-health care, sexual violence, disability, migration status, and rare conditions can expose people even when names are removed. Rules for access, consent, correction, de-identification, and breach response cannot be vague. A patient who fears exposure may avoid care entirely.
Data also has to return to the place where action is possible. A dashboard that shows missed appointments, medicine shortages, referral delays, outreach gaps, complaints, and climate-readiness problems is useful only if managers use it to correct work. Data that travels upward and never comes back leaves the clinic blind. The region does not need more numbers stored in reports. It needs information that changes decisions.
Community feedback must lead to repair. Patients and families need a simple way to report problems, but the real test comes after they speak. Was the waiting time reviewed? Was signage corrected? Was the referral instruction clarified? Was stock management improved? Was a disrespectful service pattern addressed? Was clinic communication changed? Consultation without return teaches the public that silence is more efficient than participation.
Implementation will fail if it tries to move everywhere at once. Caribbean ministries need sharper sequencing. Start where harm is high and the break is visible. In one country, chronic-care medicine stock may be the most urgent problem. In another, referral tracking after screening may be the point of failure. Elsewhere, emergency continuity for dialysis, maternity, older-person services, or psychiatric medication may need priority. The correct starting point is where patients are being harmed and where a disciplined routine can show progress.
Early wins should be concrete enough for people to notice. Fewer stock-outs. Cleaner referrals. Better follow-up for high-risk patients. Current vulnerable-patient lists. Shorter delays after screening. Clearer clinic hours. More respectful communication. These changes are not small to the patient who depends on them. They build trust because they change the service rather than the language around the service.
Fiscal honesty matters. Caribbean governments work with narrow room for waste. Donor money may help, but it cannot replace national responsibility. Regional cooperation may stretch capacity, but it cannot correct weak local management by itself. Social science may improve design, but it cannot compensate for refusal to fund the basics. A serious plan names the constraint, chooses the sequence, protects poorer households, supports workers, and measures whether care is improving.
Public reporting should speak in terms people recognize. Medicine availability. Appointment access. Referral completion. Emergency readiness. Waiting time. Patient feedback. Clinic-level correction. Ministries do not need to publish every internal failure, but they do need to show enough truth for the public to believe the system is being managed. Reporting that reads like public relations will only deepen suspicion where patients see no improvement.
Clinic managers need authority that matches the blame they receive. It is unreasonable to hold a manager responsible for stock failure, delayed repairs, poor scheduling, or missed communication when every practical decision sits elsewhere. The line between clinic, district, national, and regional authority has to be clear. A manager who cannot solve small problems will watch them grow into larger failures.
Training should change work, not attendance records. A session on NCD care means little if follow-up routines remain unchanged. Climate-health training means little if no vulnerable-patient list exists afterward. Digital-health training means little if staff return to double reporting and heavier workload. Good training leaves behind tools, checklists, supervision changes, and a different week of work.
Patient dignity must stay inside the implementation process. Registers, maps, dashboards, and screening forms can become cold instruments if the person disappears behind the record. Staff should explain why information is collected, who will see it, how referrals work, and what the patient can expect next. Dignity is not separate from efficiency. People return to services they understand and trust.
The deeper requirement is a repair culture. Every health system fails at some point. Weak administration hides the failure, blames the patient, punishes the worker, or waits for the next crisis. Better administration asks what broke, who was harmed, why the routine failed, and what will change before the same harm returns. That habit should guide supervision, management review, community feedback, and public reporting.
Management meetings need less ceremony and more evidence. The useful meeting is not the one that repeats national priorities. It is the one that reviews missed appointments, delayed referrals, stock problems, complaints, outreach gaps, climate weaknesses, and cases where delay harmed patients. A district team should leave knowing who owns each correction and when it will be checked again. Accountability is not a slogan. It is the habit of seeing failure early enough to prevent the next injury.
This implementation agenda is deliberately grounded. It does not ask Caribbean health systems to copy large-state models or announce reforms that collapse under their own ambition. It asks them to know the patient route, protect continuity, hold medicines in stock, support workers, use data carefully, connect care to social need, prepare for climate disruption, and repair what breaks. Health development becomes real when these routines change the care people receive.
Chapter 8: Final Analysis and Recommendations
Caribbean health development will not be rescued by a borrowed model, a new slogan, or another strategy document written far above the clinic. The region’s conditions are too specific for that kind of copy-and-paste reform. Small populations, island geography, climate exposure, chronic disease, professional migration, diaspora links, and close community networks all shape how care works. A policy that ignores those conditions may look impressive on paper and still collapse in the clinic, the pharmacy, the ambulance route, or the household where treatment is supposed to continue.
The stronger path is less dramatic and more demanding. Caribbean health systems need services that can be trusted in the small points of contact where patients actually meet the state. Medicine should be there when the patient returns. A referral should lead to a known destination, not uncertainty. A clinic should notice when a high-risk patient disappears. A nurse should have enough support to remain in service. A data system should help managers correct failure, not just feed reports upward. An emergency plan should identify real patients whose treatment cannot stop, not only the facilities likely to be damaged.
The study’s main finding is that health administration and social science cannot be separated in serious Caribbean reform. Chronic disease is not managed by clinical instruction alone. Food prices, transport, work schedules, fear, health literacy, family pressure, and trust all decide whether a patient follows treatment. Climate readiness is not only about buildings and supplies. It depends on knowing who lives alone, who lacks transport, who needs insulin, who depends on dialysis, who may not receive a warning, and which local messenger the community will believe. Digital health is not progress by itself. It becomes useful only when it fits the lives of older adults, rural families, low-literacy patients, migrants, and households with little privacy.
Workforce retention follows the same logic. Training more health workers will not solve much if the system keeps losing them to poor supervision, unsafe conditions, blocked advancement, weak morale, or migration pressure. A Caribbean health worker is not just a post in a staffing table. In a small system, that person may carry patient memory, local trust, informal knowledge, and the practical judgment that keeps a fragile service moving. Losing such workers weakens the system in ways that official vacancy counts rarely capture.
Primary care should become the organizing base of reform. That does not mean romanticizing community clinics or pretending they can do everything. It means giving them the tools required to carry the work already placed on them. Chronic-care registers, referral tracking, medicine forecasting, patient recall, social-risk screening, and community follow-up are not decorative administrative tasks. They are the machinery of prevention. If they fail, the hospital later receives the evidence as stroke, kidney failure, infected wounds, avoidable admissions, maternal danger, or disability that could have been prevented.
Patient continuity should be the clearest test of whether reform is working. Can a patient with diabetes obtain medicine, understand the advice, complete referral, receive review, and remain protected during a storm or service disruption? Can an older person living alone be identified before a hurricane cuts off access? Can a pregnant woman who misses follow-up be traced before risk deepens? Can a clinic tell which patients are controlled, which are slipping, and which have already been lost? Where the answer is no, the failure is not abstract. It is a management problem with human cost.
Regional cooperation remains necessary, but it has to be treated as working infrastructure rather than ceremonial language. Shared procurement, laboratory support, surveillance, training, emergency knowledge, and specialist capacity can help small states avoid paying alone for services they cannot efficiently carry by themselves. Yet cooperation only has value when it reaches the point of care. If regional purchasing lowers cost but the clinic shelf is still empty, the gain has not reached the patient. If regional surveillance produces data but local teams cannot act on it, the system has collected information without changing risk. If emergency guidance never becomes a facility routine, preparedness remains unfinished.
Data needs the same discipline. Open data and dashboards can sharpen accountability, but Caribbean privacy risks are real. In small communities, sensitive information can expose people even when names are removed. HIV status, mental-health care, disability, sexual violence, migration status, and rare conditions require careful governance. Trust will not survive a data system that makes people feel watched, exposed, or punished. Evidence should protect patients before it protects institutional image.
Community trust cannot be handled as public relations. It is built in the way staff speak to patients, the way complaints are answered, the way ministries return after consultation, and the way services correct visible problems. Churches, schools, local leaders, youth groups, diaspora networks, neighborhood associations, and family structures all shape how people receive health advice. They are not audiences waiting for instruction. They are part of the practical environment in which care succeeds or fails.
The reform language should stay modest because the work itself is difficult enough. Caribbean health systems do not need promises that sound larger than delivery. A smaller reform that improves medicine availability, referral completion, clinic recall, staff support, climate communication, or patient dignity may do more for public health than a national plan that never changes the patient’s journey. In small systems, credibility is earned quickly or lost quickly. People know when the clinic works better. They also know when nothing has changed.
This study defends a simple standard. A Caribbean health system is stronger when a poor patient can seek care without shame, when an older person is not abandoned during a storm, when a nurse has reason to stay, when a clinic can find a patient before danger deepens, when a health ministry sees failure early enough to correct it, and when public institutions keep faith with the communities they serve.
That is the real meaning of readiness. Not a longer document, louder launch, and not a borrowed framework dressed in local language. Readiness is the ability to keep care moving when money is tight, staff are stretched, disease is chronic, climate pressure is rising, and households are already carrying more than they can afford. Caribbean health development will advance when public institutions become more reliable in those conditions. The measure is not the ambition of the plan. The measure is whether people experience safer, fairer, more humane care when they need the system most.
References
Caribbean Public Health Agency. (2025). Results-oriented strategic plan 2025-2030: Stronger together: Advancing Caribbean public health. CARPHA.
CARICOM Secretariat. (2022). Strategic plan for the Caribbean Community 2022-2030. Caribbean Community.
Pan American Health Organization. (2024a). Leading causes of death and disease burden in the Americas: Noncommunicable diseases and external causes. PAHO.
Pan American Health Organization. (2024b). Open data for Caribbean health: Special issue and regional evidence use. PAHO.
Pan American Health Organization. (2024c). Trinidad and Tobago country profile: Health in the Americas. PAHO.
Pan American Health Organization. (2026). PAHO launches seven new Caribbean climate and health country profiles. PAHO.
World Bank. (2023). Noncommunicable diseases care in the Eastern Caribbean: Dominica, Grenada, and Saint Lucia. World Bank.
World Bank. (2024a). The economic impact of non-communicable diseases in the Caribbean. World Bank.
World Bank. (2024b). Health financing and resilience in Latin America and the Caribbean. World Bank.
World Bank. (2025). Current health expenditure per capita (current US$): Caribbean small states. World Development Indicators.
World Health Organization. (2023). Primary health care measurement framework and indicators: Monitoring health systems through a primary health care lens. WHO.
World Health Organization. (2024). Climate change and health: Small island developing states and health-system resilience. WHO.