

Partnership Design, Local Trust, Workforce Support, and Sustainable Delivery
Research Publication by Elijah C. Onuoha
New York Center for Advanced Research (NYCAR)
Institutional Review
June 2026
DOI: https://doi.org/10.5281/zenodo.20628693
Publication Number: NYCAR-TTR-2026-RP057
Peer Review Status: Approved for publication release. This master’s research publication meets the New York Center for Advanced Research (NYCAR) standard for applied scholarship, source discipline, APA 7th accuracy, policy relevance, and professional presentation. The paper demonstrates clear command of NGO-led healthcare delivery in African communities, with strong attention to partnership design, local accountability, workforce support, referral continuity, community trust, and sustainable service practice. Its value lies in connecting public evidence with practical management judgment, showing how NGOs can strengthen care without weakening local systems or replacing public responsibility. The work is approved as a complete research publication suitable for institutional, academic, and professional readership without appendix material.
Abstract
This master’s research publication examines building health care in NGOs in African communities in African communities where NGOs, governments, and local health workers share service responsibility. It is written for applied public-service and institutional audiences, but it does not reduce policy to a checklist. The argument begins where people meet systems: the clinic, the school, the community meeting, the household, the NGO field office, or the local government desk. The work draws on current public evidence and peer-informed policy sources, including official Nigerian health and education materials, UN strategy reports, WHO and World Bank monitoring, and institutional case evidence. The central position is that reform becomes credible only when it can be seen in routine service, measured through honest records, and corrected when users are harmed or ignored. The publication develops a practical implementation model, uses black-and-white charts and tables for decision support, and concludes with a roadmap for leaders who want change to survive beyond launch speeches.
Keywords: building; community; health; through; african; models; accountable; NYCAR; applied research; governance; policy; institutional reform
List of Tables and Figures
Table 1. NGO healthcare partnership model
Table 2. NGO project-to-system transition checklist
Figure 1. NGO health-system contribution domains.
Figure 2. Community health NGO operating mix.
Figure 3. Common sustainability risks in NGO health care.
Figure 4. Accountability channels for NGO care.
Figure 5. Implementation readiness stages.
Chapter 1: Introduction: NGO Health Care Beyond Charity
1.1 Why NGO health work must be treated as public trust
Health care delivered by NGOs in African communities is never a neutral service. It enters places where households may already have seen promises fade, clinics open without medicines, and outreach teams disappear after a funding cycle. The opening concern is not whether NGOs can help; they clearly can. The harder question is whether their work strengthens local care or leaves another short-lived project behind.
The strongest NGO health programmes begin with humility. They do not arrive as saviours, and they do not treat the public system as an obstacle to be bypassed. They study the community, listen to local workers, respect existing institutions, and identify where the gap is specific enough for useful action. That discipline prevents charity from becoming performance.
The paper therefore frames NGO health care as a responsibility of trust. Communities judge programmes by whether care appears when promised, whether staff speak with respect, whether referral works, whether medicines are available, and whether complaints are heard. These ordinary encounters decide whether an NGO becomes a partner or another visiting name on a banner.
1.2 Reading evidence beside community reality
Evidence in community health must be read with a field sense. National data can show maternal risk, financing pressure, workforce shortage, or poor service coverage, but it cannot by itself explain why one village avoids a clinic, why one district has repeated stock-outs, or why a project struggles after donor visits end. The value of evidence lies in how well it guides local decisions.
Public health reports, NGO records, and community testimony should be placed beside one another. When those sources agree, managers can act with greater confidence. When they differ, the difference itself becomes useful. A high reported coverage rate means little if families still describe payment barriers, poor attitude, insecurity, or referral delays. Numbers should sharpen questions, not close them too early.
Professional judgement is needed because NGO health work sits between public policy and daily hardship. The best managers avoid broad claims that cannot be proved. They ask what service is missing, who is excluded, what local capacity already exists, which actor is responsible, and how the programme will leave behind stronger practice rather than dependency.
1.3 Management decisions that shape credibility
Outcomes in NGO health care are often decided before the outreach day begins. A manager chooses the district, the local partner, the staffing pattern, the supply route, the supervision rhythm, the reporting method, and the handover plan. Each choice either builds credibility or creates a weakness that later appears as poor attendance, unused equipment, weak referral, or community suspicion.
A serious NGO programme should be able to answer direct operational questions. Who approves the work plan? Who tracks medicine use? Who confirms that community health workers are supervised? Who meets the local health authority? Who follows up on referred patients? Who corrects a failed activity? If those answers are unclear, the programme may look active while drifting below the standard of responsible care.
The management lesson is plain: good intentions do not manage a health service. Reliable service requires named authority, written records, fair staff treatment, community feedback, and a budget that reflects what the work actually costs. Without those controls, the project may satisfy a donor report while failing the people whose trust it borrowed.
1.4 Guardrails against dependency, waste, and harm
NGO work carries risk as well as value. It can duplicate public services, draw staff away from government facilities, create community expectations that cannot be sustained, or focus on visible outputs while ignoring continuity. These risks do not make NGOs harmful by nature. They show why governance has to be built into the project from the start.
The safest programmes protect three lines at once: community dignity, public-system connection, and financial accountability. Dignity requires respectful care and honest communication. Public-system connection requires coordination with local authorities and facility teams. Financial accountability requires clear spending records, procurement discipline, and evidence that resources reached the intended service.
A programme that cannot be sustained should say so honestly. Temporary work may still be valuable in emergencies, fragile settings, or remote settlements, but it should not pretend to be permanent. The ethical standard is candour: tell the community what the project can do, what it cannot do, and how local actors will be supported when the NGO reduces its presence.
Figure 1. NGO health-system contribution domains.
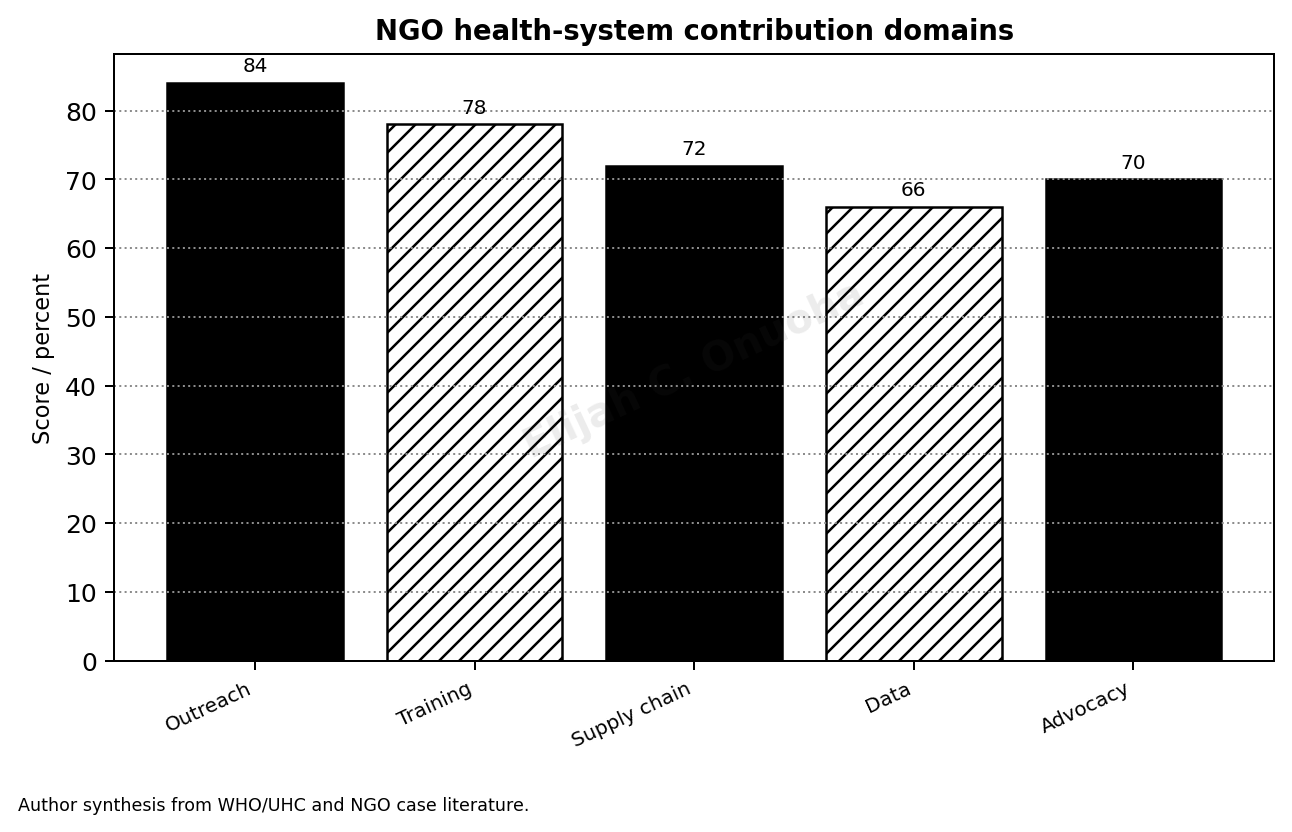
Source: Author synthesis from WHO/UHC and NGO case literature.
Chapter 2: African Community Health Needs and Institutional Gaps
2.1 Health need as lived pressure, not a statistical label
African community health needs are often described through indicators: mortality, disease burden, service coverage, immunisation, nutrition, and health expenditure. Those indicators matter, but they become meaningful only when connected to household life. A mother who delays care because transport is unsafe, a child who misses treatment because the clinic has no medicine, and an older patient who cannot return for follow-up all reveal the real shape of need.
NGOs often enter communities where public services exist but do not function dependably. The building may be present, the staff may be few, the record book may be incomplete, and the referral link may be weak. In such settings, the problem is not only absence. It is partial presence: enough structure to raise hope, not enough service to protect people reliably.
The argument is strongest when it treats health need as pressure on a whole local system. Disease is clinical, but access is social. Cost, distance, gender norms, insecurity, trust, staffing, and supply shape whether the clinical answer reaches the person who needs it.
2.2 Interpreting data without losing the ground view
The data used in African community health studies must be handled with care. Household surveys, NGO activity reports, government figures, and global monitoring documents each carry value, but each has limits. Survey data may lag behind current conditions. NGO reports may favour activities the project funded. Facility records may undercount people who never arrived. A careful scholar reads across these limits.
Global monitoring on universal health coverage and financial protection shows why community health cannot be separated from cost and service availability (World Health Organization & World Bank, 2025). Yet an African programme still needs local verification: which households are missing care, which services fail regularly, which routes are unsafe, and which providers have lost public confidence.
Evidence should lead to better management questions. A low antenatal-care completion rate may point to distance, cost, poor treatment by staff, lack of male support, or weak follow-up. A single indicator rarely identifies the full cause. Good NGO leadership treats data as an entry point for inquiry, not as a substitute for inquiry.
2.3 Gaps between local capacity and project ambition
Many NGO programmes fail because project ambition grows faster than local capacity. A proposal may promise outreach, training, referral, health education, data reporting, and service improvement across many settlements. The local team may have one supervisor, unreliable transport, limited storage, weak internet, and workers already stretched by routine duties. The gap between the plan and the capacity then becomes the real project.
A careful programme design should ask what the community can absorb without distortion. Can the health facility receive the additional referrals? Can trained volunteers continue after stipends end? Can the local government maintain supplies? Can the data system be used by the people who collect the data? Ambition that ignores these questions becomes a burden placed on fragile systems.
Partnership with public authorities is not a ceremony. It is the mechanism through which temporary support can become stronger local practice. If a project improves maternal referral, disease surveillance, nutrition screening, or community follow-up, the public system should be involved early enough to own the routine after donor financing changes.
2.4 Equity risks in community programmes
Community health projects can widen inequality when they are not deliberately designed. Programmes may favour accessible villages, communities with active leaders, areas near roads, or groups that are easier to document. The most isolated households may remain outside the service even while aggregate project numbers look impressive. Equity requires managers to search for the people who are least visible.
Gender, disability, age, displacement, language, and poverty all shape access. A health talk in a central venue may not reach women who cannot leave home, people with mobility limitations, informal workers who cannot lose a day’s income, or minority-language groups. NGO planning has to move beyond attendance numbers and ask who could not attend, who did not speak, and who was never invited.
Safeguards should be practical. Outreach maps, disability-sensitive referral, female community mobilisers, grievance channels, local translation, and transport support can make a visible difference. The aim is not to make the report look inclusive; it is to make the service harder to miss for people who usually remain outside the count.
Figure 2. Community health NGO operating mix.
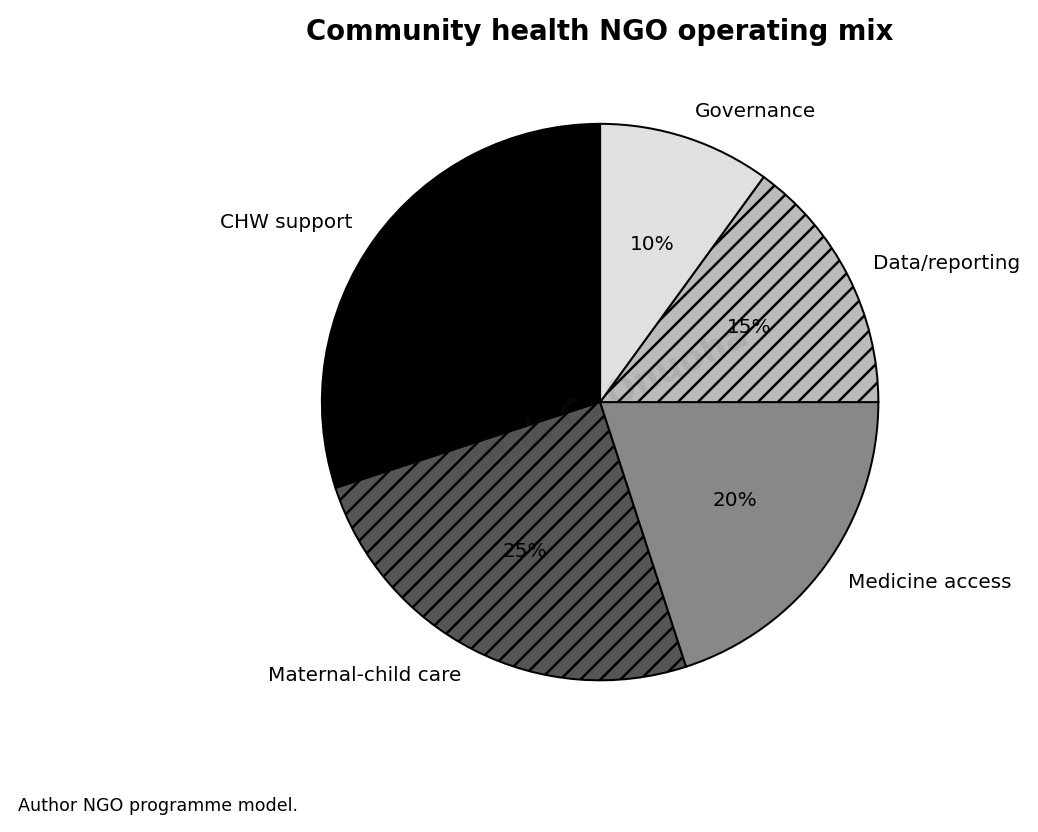
Source: Author NGO programme model.
Chapter 3: Partnership Design Between NGOs and Public Systems
3.1 Partnership as shared work with clear authority
Partnership is one of the most repeated words in NGO health care, yet it is often the least disciplined. A meeting, memorandum, or photograph does not prove partnership. Real partnership means that roles are clear, decisions are recorded, staff know who supervises whom, money is traceable, and local authorities are not surprised by activities carried out in their communities.
NGOs and public health systems bring different strengths. NGOs may move quickly, attract donor funding, test community models, and reach neglected areas. Public systems carry legal mandate, facilities, health workers, data responsibility, and long-term duty. The danger appears when either side treats the other as a decoration. Partnership must connect speed with legitimacy.
A strong partnership agreement should answer basic questions before work begins: the service package, the site selection logic, staff roles, referral route, procurement method, reporting schedule, safeguard procedure, and exit plan. When these questions are answered late, tension is almost guaranteed.
3.2 Choosing partners and sites with evidence
The choice of community, facility, and partner determines much of the project’s moral quality. Selecting places because they are easy to reach may improve activity numbers while leaving the hardest communities untouched. Selecting partners because they are politically convenient may weaken professional judgement. Site selection should be defensible through need, feasibility, risk, and equity.
Public data can identify underserved areas, but local verification should follow. A community listed as covered may lack regular staff. A facility counted as functional may lack essential drugs. A district with active NGOs may still have poor referral or weak trust. The selection process should include health workers, community representatives, local government, and people who know the unofficial barriers.
Partner due diligence should also be serious. Goodwill is not enough. A local organisation should be assessed for financial controls, community reputation, safeguarding practice, staff capacity, and ability to report honestly. A weak partner can damage the programme faster than a weak budget.
3.3 Contracts, referral, and supervision choices
Project contracts should not be written only for donors and lawyers. They should guide the field. Staff and partners need to know what service is promised, which standard applies, how incidents are reported, how supplies are tracked, and how complaints move. A contract that cannot be translated into daily work becomes a document kept far from the place where care happens.
Referral deserves special attention. Many community projects identify illness without being able to complete the path to treatment. Screening a child, identifying danger signs in pregnancy, or diagnosing a chronic condition is not enough if the patient cannot reach a facility that is ready to respond. Referral should include transport logic, receiving-facility contact, feedback to the community worker, and follow-up with the household.
Supervision is the quiet discipline that protects quality. Without it, training fades, records become unreliable, and community workers begin improvising beyond their competence. Supervision should be regular, supportive, and evidence-based. The aim is correction, not intimidation.
3.4 Avoiding parallel systems
NGO programmes sometimes build parallel systems because they want speed. They create separate registers, separate supply chains, separate incentives, and separate reporting lines. This can solve a short-term problem while weakening the public system that will remain after the project ends. Parallelism is convenient at the beginning and costly at the end.
Not every separate arrangement is wrong. In emergencies, displacement settings, or areas of severe state failure, an NGO may need temporary systems to protect life. The problem arises when temporary systems become the normal way of working without a plan for alignment. If local health authorities cannot use the data, supplies, training records, or referral habits, the programme is leaving too little behind.
A better approach is deliberate connection. Project records should feed local planning. Training should involve facility supervisors. Supplies should be tracked in ways public managers can understand. Community committees should be linked to existing local structures. The goal is not to make the NGO invisible; it is to make the improvement durable.
Figure 3. Common sustainability risks in NGO health care.
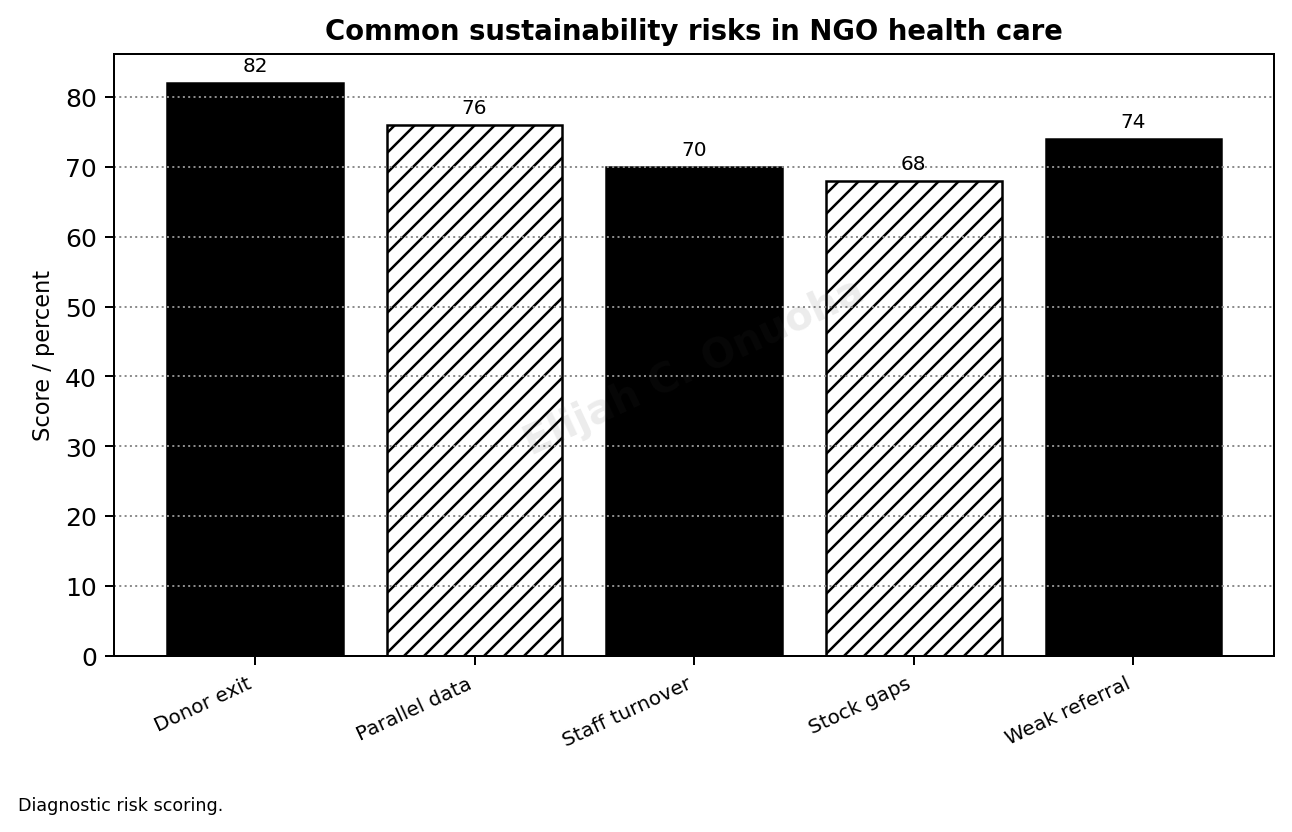
Source: Diagnostic risk scoring.
Read also: Rural Health Policy That Works: Local Government Renewal for Primary Care in Nigeria
Chapter 4: Community Health Workers and Local Trust
4.1 Community health workers as the public face of care
Community health workers often become the most trusted face of a health programme. They know households, language, terrain, customs, and the small signs of fear or hesitation that formal systems miss. Their value is not only technical. They carry relationship. In communities where distant institutions are mistrusted, that relationship may be the difference between early care and dangerous delay.
The mistake many programmes make is to praise community health workers while under-supporting them. They are asked to educate, screen, refer, report, mobilise, follow up, and calm complaints, often with modest pay and irregular supervision. Admiration does not replace transport, supplies, training, and protection. A programme that depends on them must invest in them.
Community trust should be treated as a service asset. It is built through repeated reliability: showing up, keeping records, respecting households, admitting limits, and following through after referral. Trust can be lost quickly when workers are sent into the field without the backing to solve what they are asked to notice.
4.2 Training that respects limits and responsibility
Training is often counted as an output, but the number trained does not prove capacity. A two-day workshop may raise awareness without changing practice. Effective training for community health workers must be specific, repeated, supervised, and tied to tasks they are allowed to perform. It should clarify not only what to do but when to refer and when to stop.
Clinical boundaries matter. Community workers should not be pushed into roles that require professional qualification simply because the formal system is thin. Their strength lies in health promotion, early warning, basic screening, follow-up, adherence support, referral encouragement, and community feedback. When programmes expand their role without safeguards, risk is transferred to the worker and the household.
Training should also include dignity, confidentiality, gender sensitivity, disability awareness, and complaint handling. These subjects are sometimes treated as softer than clinical content. In community work they are central. A technically correct message delivered without respect can close the door to future contact.
4.3 Incentives, recognition, and accountability
Community health work cannot rest on sacrifice alone. Some programmes rely on volunteers because budgets are tight, but unpaid or poorly paid labour creates instability and unfairness. People who carry public-health responsibility need reasonable compensation, transport support, protective materials, recognition, and a pathway for learning. Otherwise attrition becomes predictable.
Incentives should be designed carefully. Payment only for activity counts can encourage inflated numbers. Payment only for attendance can ignore quality. Non-financial recognition can help but cannot substitute for fair support. The best systems combine modest financial stability with supervision, respectful treatment, and clear expectations.
Accountability must be balanced. Community health workers should report accurately and respect boundaries, but supervisors also owe them timely guidance, supplies, and protection from unsafe demands. A one-sided accountability system blames the weakest actor while ignoring decisions made above them.
4.4 Safeguards against overburdening the front line
The front line becomes overburdened when every new project adds another form, another target, another message, and another meeting. Community workers may then spend more time proving activity than supporting households. The effect is subtle: the programme appears organised, but the person closest to the community is exhausted and less available for meaningful contact.
Managers should review workload before adding tasks. If a worker is already covering maternal health, nutrition, immunisation follow-up, malaria education, and referral, another reporting requirement may reduce quality. Good management protects attention. It asks which task matters most, which can be combined, and which should be removed.
Safeguards include task limits, simple records, regular debriefing, mental health awareness, and escalation routes when workers meet problems they cannot solve. Community health workers should not be left carrying the emotional weight of poverty, illness, and system failure without professional backing.
Figure 4. Accountability channels for NGO care.
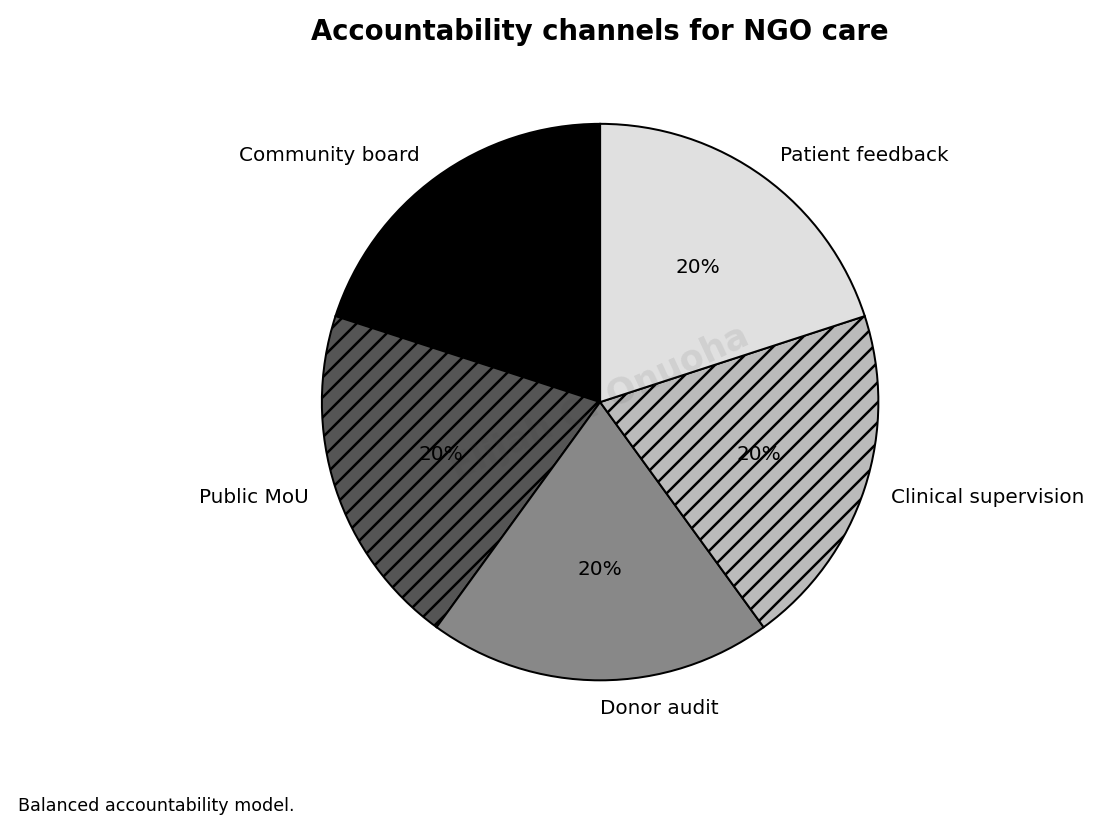
Source: Balanced accountability model.
Table 1. NGO healthcare partnership model
| Partnership area | Required practice | Why it matters |
| Government alignment | Formal MoU with LGA/state health actors | Prevents parallel systems |
| Community voice | Village health committee and patient feedback | Builds legitimacy |
| Clinical quality | Supervision and referral rules | Protects safety |
| Finance | Transparent project budget and transition plan | Reduces donor-dependence shock |
| Data | Shared indicators with public facilities | Improves continuity |
Note. Table prepared for NYCAR publication format.
Chapter 5: Maternal, Child, Nutrition, and Primary Care Programmes
5.1 Maternal and child health as the test of reach
Maternal and child health reveals whether an NGO programme can move beyond intention. A pregnancy complication, a newborn illness, or a malnourished child does not wait for institutional convenience. The service has to reach the household early, speak in a language the family trusts, connect to a facility, and reduce the cost and delay that often turn risk into tragedy.
Programmes in this area must connect health education with service readiness. Telling women to attend antenatal care is weak if the facility is disrespectful, under-supplied, far away, or costly. Encouraging skilled birth attendance matters, but the referral path must be real. The message and the service must meet.
The management task is to align community mobilisation, facility capacity, transport, nutrition support, immunisation follow-up, and emergency referral. Each part may be small in a work plan, but families experience them as one chain. When one part fails, the whole intervention loses force.
5.2 Evidence on vulnerability and service contact
Maternal, child, and nutrition indicators in African communities are shaped by income, distance, education, gender power, conflict, and the strength of primary care. Public data can identify broad risk, but project design still needs local attention to who is missing from services. The families most at risk may also be those least likely to appear in routine facility numbers.
Nigeria’s demographic and health evidence shows why maternal and child services remain urgent, while global UHC monitoring keeps attention on service coverage and financial hardship (National Population Commission & ICF, 2025; World Health Organization & World Bank, 2025). An NGO programme should use such evidence to select priorities, not to decorate a proposal already written.
The most useful evidence is actionable. Which settlement has low antenatal attendance? Which facility reports repeated stock-outs? Which households default after referral? Which children are missed by immunisation follow-up? A manager who can answer those questions has a better chance of correcting service failure before it becomes severe harm.
5.3 Coordinating nutrition, immunisation, and referral
Nutrition, immunisation, antenatal care, malaria prevention, and referral are often managed as separate activities because donors and programmes divide them that way. Households do not. The same child may need nutrition screening, vaccination follow-up, fever treatment, and caregiver education. The same mother may need antenatal care, transport planning, and support for safe delivery. Integration should be practical, not rhetorical.
A joined approach begins with the field schedule. If outreach teams visit a community, the visit should be planned around real household needs rather than programme silos. Records should allow a worker to see missed immunisation, malnutrition risk, and maternal danger signs without creating an impossible paperwork burden. The receiving facility should know what referrals to expect.
The most effective coordination is quiet. It appears in a shared register, a working phone number, a supervisor who checks unresolved cases, and a facility that recognizes referrals from community workers. These small habits determine whether a programme becomes care or only activity.
5.4 Avoiding the weakness of vertical campaigns
Vertical campaigns can achieve quick gains. They can focus attention, gather supplies, and mobilise a large number of people around a specific disease or service. The weakness appears when campaigns end and routine care remains unchanged. Communities may receive a burst of attention followed by silence. That cycle damages confidence.
The risk is not the campaign itself. The risk is campaign thinking. A programme that treats each health problem as a separate event can miss the household’s continuing needs. A child treated for malaria may still need nutrition support. A woman reached during a maternal-health campaign may still need transport and respectful facility care. The campaign should open the door to continuity.
NGO managers should design campaigns with routine service in mind. Every campaign should ask what will remain: trained staff, better referral habits, cleaner records, community knowledge, supply discipline, or stronger supervision. If the answer is unclear, the project may be highly visible and still strategically weak.
Figure 5. Implementation readiness stages.
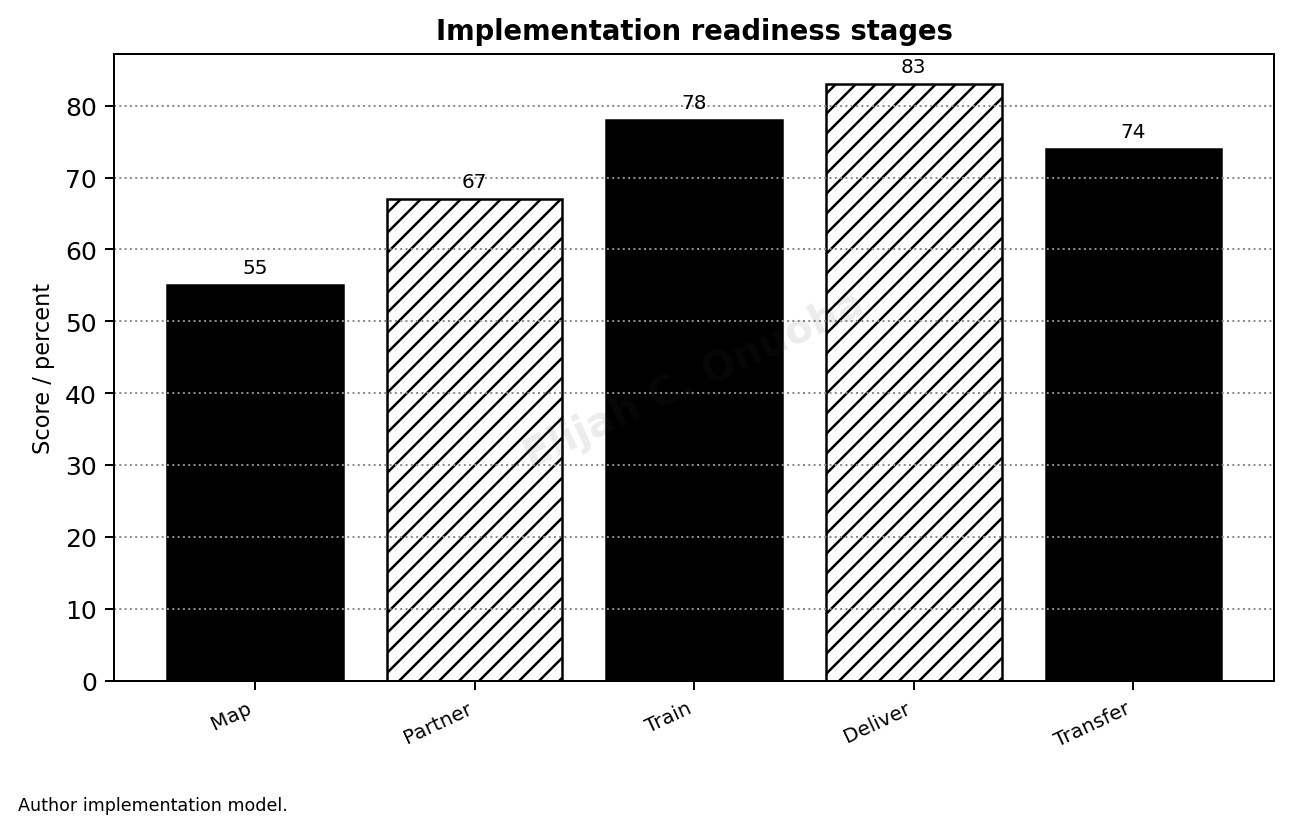
Source: Author implementation model.
Chapter 6: Supply Chains, Data, and Mobile Outreach
6.1 Medicines and logistics as proof of seriousness
Supply chains decide whether promises become care. A community meeting can raise awareness, but confidence collapses when families reach the facility and find essential medicines absent. In NGO health work, logistics is not a technical side issue. It is the visible proof that management respects the time, money, and hope of the people it calls to service.
Strong supply management begins with realistic forecasting. Managers need to know the population, disease pattern, service package, storage condition, transport route, and likely demand. Procurement that ignores these factors produces either stock-outs or waste. Both weaken trust. Medicines that expire in storage and medicines missing at the point of care are two sides of the same failure.
NGO programmes should share supply information with local authorities and facility teams. If the project creates a separate supply route, it should still build records that can be audited and learned from. The aim is not only to deliver commodities; it is to strengthen the habit of reliable availability.
6.2 Data that leads to correction
Data collection has become one of the busiest parts of NGO health work. Forms, registers, dashboards, and mobile tools can improve visibility, but they can also bury staff under reporting requirements that do not change decisions. Data becomes valuable only when someone uses it to correct service failure.
A practical data system should answer a limited set of management questions. Which service is being used? Which community is under-reached? Which referral is unresolved? Which medicine is running low? Which staff member needs support? Which complaint is recurring? These questions are more useful than a large report that arrives too late to guide action.
Digital tools should be judged by field usefulness. A mobile reporting application that fails in low-connectivity areas, duplicates paper work, or produces numbers that local managers cannot interpret will frustrate the people it claims to help. The test is not whether the tool looks modern; it is whether it improves decision, follow-up, and accountability.
6.3 Mobile outreach with a referral backstop
Mobile outreach can reach people who are far from facilities, displaced by conflict, restricted by poverty, or excluded by terrain. It is one of the practical strengths of NGO health care. Yet outreach without referral can become a moving announcement of unmet need. Screening, counselling, and basic treatment should be connected to a path for cases that require higher care.
A good outreach plan identifies the receiving facility before the team leaves. It clarifies transport options, referral criteria, communication with facility staff, and follow-up responsibility. The community should not be left with a referral note that nobody expects to honour. A referral system that stops at advice is incomplete.
Outreach should also respect community rhythm. Market days, farming seasons, religious activities, school schedules, and security conditions affect attendance. Field teams that ignore local timing may misread low turnout as apathy. In many communities, timing is part of access.
6.4 Risks in stock, data, and outreach systems
Supply, data, and outreach systems carry their own risks. Medicines may leak, records may be inflated, outreach may favour accessible communities, and data tools may create pressure to count rather than care. A serious NGO does not wait for scandal before building safeguards. It assumes that systems need checks because pressure, fatigue, and incentives can distort practice.
Safeguards should be simple enough to use. Stock cards, spot checks, supervisor review, community verification, incident reports, and referral audits can prevent many failures. Complex controls that field teams do not understand can become another source of disorder. The goal is disciplined visibility.
The ethical issue is sharp. Communities are often asked to trust programmes with their health, data, time, and private information. Mismanaged records or weak supplies can expose them to harm. Responsible management treats logistics and data as matters of dignity, not administrative housekeeping.
Chapter 7: Financing, Donor Accountability, and Exit Risk
7.1 Donor funding and the cost of continuity
Donor funding can open services that would otherwise not exist. It can support outreach, train workers, buy supplies, and test new delivery models. The danger is that a project may create a level of service the local system cannot continue. When funding ends, the community experiences withdrawal as abandonment, even if the project met its formal targets.
Continuity should be discussed at the proposal stage. Which activities are temporary? Which will be handed to local authorities? Which require recurrent financing? Which roles depend on donor stipends? Which supplies must be purchased after the project closes? These questions are not pessimistic. They protect the community from being offered a promise that cannot survive.
A responsible NGO should price the real cost of continuity. Training without supervision is incomplete. Equipment without maintenance is fragile. Referral without transport support is weak. Community mobilisation without a service response can create anger. Budget honesty is one of the clearest signs of management integrity.
7.2 Financial accountability and public confidence
Financial accountability is not only a donor requirement. It is part of public trust. Communities notice when project vehicles arrive, staff are paid, supplies appear, or promises remain unfunded. Local workers notice when allowances are delayed or resources are unevenly distributed. Money tells a story about seriousness.
Reports should make spending understandable in relation to service. How much reached community activities? How much supported supervision? How much went to procurement? How much was absorbed by administration? What service result followed? A budget line is not enough. Leaders should be able to connect money to credible field action.
Financial protection for households also belongs in this discussion. An NGO that delivers health education but ignores user fees, transport cost, and informal payments may overestimate its effect. Families may understand the message and still be unable to act. Good health management follows the cost barrier into the household, not only the clinic.
7.3 Exit planning and public-system ownership
Exit planning is often delayed because it feels uncomfortable. It should be one of the earliest conversations. A project that begins without an exit discipline may build habits that depend entirely on donor money. Staff, volunteers, local officials, and communities may then organize themselves around support that will disappear.
Public-system ownership cannot be announced at the closing ceremony. It has to be built through joint planning, shared supervision, compatible records, and gradual transfer of responsibilities. Local authorities should know the programme well before they are asked to inherit it. Facility teams should have practised the routines while the NGO is still available to support correction.
A dignified exit leaves capacity, not confusion. It leaves trained people who are still supervised, records that local managers can use, referral habits that continue, and a community that understands what has changed. A project that ends with silence teaches people not to believe the next project.
7.4 Fiduciary risk, power, and community voice
Health funding creates power. Those who control money can shape priorities, staff behaviour, and the community’s understanding of what matters. Fiduciary risk is therefore not limited to fraud. It includes distorted priorities, weak procurement, excessive administrative spending, poor transparency, and decision-making that excludes the people affected by the programme.
Community voice can reduce some of these risks when it is treated seriously. A complaint box is weak if nobody reads it. A community meeting is weak if only local elites speak. Feedback is useful when it reaches a decision forum and produces visible correction. People should see that speaking changes something.
The safeguard is not suspicion for its own sake. It is disciplined stewardship. Donor funds, public trust, staff time, and community patience are all scarce. An NGO that spends them poorly harms more than its own reputation; it damages the next organisation that asks the community to believe.
Chapter 8: NGO Health-Care Governance Model
8.1 A governance model for community delivery
The governance model proposed in this paper begins from a practical claim: community health care becomes reliable when authority, evidence, resources, supervision, and community voice meet at the service point. If any one of these is missing, a programme may look active while remaining weak. The model is meant to help leaders see those links before failure becomes visible.
The model does not pretend that every NGO programme should be identical. Emergency relief, maternal health, chronic disease support, nutrition, disability services, and mobile outreach require different methods. What they share is the need for clear responsibility, service evidence, resource discipline, and a route for correction. These features make programmes governable.
For African communities, governability matters because many projects operate where institutions are already strained. A loose project can add confusion. A well-managed project can strengthen public confidence. The difference lies in whether the NGO understands its role as part of a wider health system, not a substitute for it.
8.2 Evidence chain for management review
A useful governance model needs an evidence chain. The chain begins with community need, moves to service design, follows resource allocation, checks delivery, records outcomes, listens to feedback, and returns to management for correction. This is not a long bureaucratic ritual. It is the minimum discipline needed to know whether the project is working.
Each link should produce evidence that can be reviewed. Need can be shown through data and local testimony. Service design can be shown through the work plan. Resource allocation can be shown through budgets and procurement records. Delivery can be shown through service registers and supervision notes. Feedback can be shown through complaints, interviews, and community meetings.
The chain is broken when evidence is collected for reporting but not for decision. Many projects have data, yet still repeat the same mistakes. A mature programme asks a harder question at every review meeting: what did we learn that changes the next month’s work?
8.3 Performance meetings that lead to correction
Performance meetings should not become ceremonies. They should be short enough to remain useful and serious enough to change action. The best meetings review a small number of indicators, unresolved referrals, stock issues, staff concerns, community complaints, and next steps. A meeting that produces no correction is only a conversation.
Leadership discipline appears in the questions asked. Why did one community receive fewer visits? Why did referrals fail? Why were supplies late? Why did women avoid the facility after outreach? Why is a volunteer leaving? These questions may be uncomfortable, but they protect the programme from drifting into self-praise.
Correction should be documented. The responsible person, action, date, and follow-up evidence should be clear. This protects field staff from vague blame and protects communities from repeated promises. Accountability becomes fairer when the record shows who was expected to do what.
8.4 Balancing control with field discretion
Control is necessary in NGO health care, but over-control can damage field judgement. Central offices may demand uniform forms, fixed schedules, and standard messages, while local teams face floods, insecurity, market days, language barriers, or unexpected disease patterns. Good governance gives field teams room to adapt without losing accountability.
The balance lies in defining what is non-negotiable and what can vary. Safeguarding, financial rules, clinical boundaries, data integrity, and respect for patients should remain fixed. Timing, community entry method, local communication style, and outreach sequence may need adaptation. A programme that cannot make this distinction will either become rigid or careless.
Field discretion should be earned and recorded. Local teams should explain why a change was made, what evidence supported it, and what result followed. This turns adaptation into learning rather than improvisation hidden from management.
Table 2. NGO project-to-system transition checklist
| Phase | Management decision | Evidence to keep |
| Entry | Needs assessment and local consent | Community map and baseline |
| Delivery | CHW training and supply plan | Service logs |
| Integration | Public reporting and referral link | Joint review minutes |
| Exit | Capacity handover and finance plan | Signed transition record |
Note. Table prepared for NYCAR publication format.
Chapter 9: Implementation Roadmap for African Communities
9.1 From selection to reliable service
Implementation begins with choosing the problem carefully. A programme should not begin by asking what activity can be funded. It should ask which service failure is causing harm, which community is affected, what local capacity exists, and what the NGO can responsibly improve. Good implementation starts with disciplined selection.
After selection, leaders should prepare the service route. Community entry, staffing, supply, referral, supervision, data, safeguarding, and feedback should be arranged before public promises are made. Communities have often heard too many announcements. Another promise without readiness deepens mistrust.
Reliable service grows through repetition. The outreach team arrives when expected. Supplies match the service package. Referrals receive attention. Supervisors appear. Records are used. Complaints are answered. These habits may sound ordinary, but in fragile settings they are the substance of trust.
9.2 Evidence for implementation decisions
Implementation evidence should be close to the work. Monthly data that arrives too late to correct a stock-out or referral failure has limited value. Managers need a rhythm that allows them to see problems while they can still act. That means combining routine reports with supervisor notes, community feedback, and exception alerts.
Indicators should be few enough to matter. A project may track service use, missed communities, referral completion, medicine availability, worker supervision, household cost barriers, and complaints. Too many indicators can blur attention. Too few can hide failure. The right measure is one that leads to a decision.
Evidence also needs interpretation. A rise in service attendance may mean trust is improving. It may also mean a temporary incentive pulled people in without solving care quality. A fall in attendance may mean poor mobilisation, seasonal migration, insecurity, fees, or disrespectful treatment. Managers must resist easy explanations.
9.3 Roles, schedules, and field discipline
Implementation fails when responsibility is vague. Every major task should have an owner: community entry, clinical supervision, supply tracking, referral follow-up, finance, safeguarding, data review, and public-system coordination. Shared work is valuable, but shared work still needs named responsibility.
Schedules should reflect field reality. A plan that ignores rainy seasons, market days, insecurity, religious calendars, staff leave, and transport time is not serious. Field discipline is not rigidity. It is preparation that respects the conditions under which staff and households actually operate.
Supervisors should check both compliance and judgement. Did the team follow the agreed process? Did they adapt wisely where local conditions required it? Did they record the change? Did the change improve care? Implementation becomes stronger when supervision teaches better judgement rather than only checking boxes.
9.4 Course correction and transition risk
No implementation plan survives unchanged. Communities respond in unexpected ways, supply routes fail, local politics shift, staff resign, and evidence reveals gaps. The mark of good management is not the absence of difficulty. It is the speed and honesty with which difficulty is handled.
Course correction should be normal. A referral route may need a different facility. A training method may need revision. A community entry plan may need new leaders. A budget line may need reallocation. The programme should have enough governance discipline to make such changes without hiding them from donors, authorities, or communities.
Transition risk must be reviewed throughout implementation. The longer a programme runs, the more people depend on it. Leaders should know which activities can be handed over, which require continued donor support, and which should be closed carefully. The community deserves clarity before the final month arrives.
Chapter 10: Conclusion: From Project Delivery to Accountable Community Care
10.1 What the study establishes
This study establishes that NGO health care in African communities should be judged by the strength it leaves in local care, not by the noise it makes during a funding cycle. Outreach, training, supplies, and community mobilisation are valuable only when they connect to reliable service, accountable management, and public-system learning.
The paper’s central contribution is the insistence that NGO health work must be managed as a form of public responsibility. It may be funded privately, charitably, or through international partners, but it touches public welfare. That gives it a duty to be honest, disciplined, respectful, and accountable.
The paper rejects the romance of charity without rejecting the value of NGOs. Many communities need NGO support because public systems are underfunded or absent. The question is how that support can strengthen dignity and capacity rather than create another layer of temporary dependence.
10.2 What leaders should carry forward
Leaders should carry forward a simple standard: the programme must make care more dependable for the people it claims to serve. If it trains workers, those workers should be supervised. If it screens patients, referral should be real. If it collects data, decisions should change. If it mobilises communities, services should be ready to receive them.
The public system should not be treated as an afterthought. Even where government capacity is weak, it remains central to continuity. NGOs should work with facility managers, local authorities, professional staff, and community structures in ways that leave records, routines, and accountability behind.
Donors also have a role in better management. They should reward honesty about limits, support supervision and operating costs, and avoid forcing projects into short reporting cycles that favour visibility over reliability. A beautiful activity report is not the same as a strengthened health system.
10.3 Professional judgement as discipline
Professional judgement is the thread that holds the study together. NGO health leaders work in imperfect settings. Data may be incomplete, public systems may be weak, roads may be difficult, and community trust may be fragile. The temptation is to simplify the story. The better response is to make judgement visible and responsible.
Responsible judgement asks what can be proved, what remains uncertain, who may be harmed, what trade-off is being accepted, and how the programme will learn. It does not hide behind donor language or technical vocabulary. It speaks plainly because the people affected by decisions deserve clarity.
This discipline also protects staff. Field teams should not be asked to carry impossible promises. Community workers should not be blamed for failures built into project design. Local partners should not inherit systems they were never prepared to run. Better judgement begins by assigning responsibility fairly.
10.4 Final position
The final position is that NGO health care in African communities must move from project activity to accountable community care. The difference is not cosmetic. Project activity counts what was done. Accountable community care asks whether what was done made service more trustworthy, more reachable, more affordable, and more likely to continue.
A strong NGO does not measure success only by workshops, visits, or distributions. It asks whether people received care with dignity, whether local workers became stronger, whether public systems gained useful routines, and whether the community can see a fair account of the work. These are harder measures, but they are closer to truth.
The paper closes with a practical demand. Health programmes should leave less confusion than they found, less distance between promise and service, and more capacity in the hands of the people who will remain when the project team leaves. That is the standard by which NGO health care should be judged.
References
Agency for Healthcare Research and Quality. (2023). TeamSTEPPS 3.0. U.S. Department of Health and Human Services. https://www.ahrq.gov/teamstepps-program/index.html
Amref Health Africa. (2024). Annual report. https://amref.org/
Federal Ministry of Health and Social Welfare. (2025). FG approves N32.9bn disbursement, unveils BHCPF 2.0 to strengthen primary healthcare accountability. https://health.gov.ng/
Federal Republic of Nigeria. (2022). National Health Insurance Authority Act, 2022. Government Printer.
Last Mile Health. (2024). Annual report. https://lastmilehealth.org/
Medecins Sans Frontieres. (2025). International activity report. https://www.msf.org/
National Population Commission & ICF. (2025). Nigeria Demographic and Health Survey 2023-24: Key indicators report. DHS Program. https://dhsprogram.com/
National Primary Health Care Development Agency. (2026). Basic Health Care Provision Fund. https://nphcda.gov.ng/bhcpf/
World Bank. (2026). World Development Indicators: Nigeria health expenditure. https://data.worldbank.org/
World Health Organization & World Bank. (2025). Tracking universal health coverage: 2025 global monitoring report. https://www.who.int/publications/i/item/9789240117808
World Health Organization. (2025). State of the world’s nursing 2025. https://www.who.int/publications/i/item/9789240110236