

Financing, Workforce Reliability, Referral Readiness, and Household Protection
Research Publication by Kevin I. Onyeberechi
New York Center for Advanced Research (NYCAR)
Institutional Review
Date: June 2026
Publication Number: NYCAR-TTR-2026-RP054
DOI: https://doi.org/10.5281/zenodo.20626902
Peer Review Status: Approved for publication release. This master’s research publication meets the New York Center for Advanced Research (NYCAR) standard for applied policy scholarship, source discipline, APA 7th accuracy, practical relevance, and professional presentation. The paper demonstrates a clear command of rural health policy in Nigeria, with strong attention to primary care readiness, local government responsibility, health financing, workforce access, maternal referral, and household protection. Its contribution lies in connecting public evidence with practical governance judgment, showing how rural health reform can become visible in the daily experience of communities rather than remain confined to national policy language. The work is approved as a complete research publication suitable for institutional, academic, and professional readership without appendix material.
Abstract
This master’s research publication examines rural health policy as a local-government delivery problem in Nigeria. It argues that rural communities benefit when policy is tested at the point where households actually seek care: the primary health centre, the maternity referral route, the community health post, the claims desk, the drug shelf, the transport link, and the ward committee that should hear complaints before avoidable harm becomes routine. The study treats rural health as a chain of service conditions involving finance, staffing, supervision, medicine availability, data use, insurance protection, referral readiness, and community trust. It draws on Nigerian health-sector law, the National Health Insurance Authority Act, Basic Health Care Provision Fund materials, Nigeria demographic and health reporting, World Bank health-financing indicators, and World Health Organization materials on primary care, universal health coverage, and the health workforce. The central position is practical: rural health renewal will not be achieved by national declarations alone. It will be achieved through facilities that open reliably, workers who can remain in post with dignity, funds that reach service points, referral routes that complete care, insurance that reduces cash pressure, and records that make local government answerable for what families experience.
Keywords: rural health policy; Nigeria; local government; primary health care; BHCPF; NHIA; health workforce; maternal referral; household protection; public accountability; NYCAR
Contents
Introduction: Rural Policy at the Point of Care
Nigeria’s Rural Health Burden and Local Government Responsibility
Primary Health Care Funding and the BHCPF Pathway
Rural Workforce, Community Health Workers, and Retention
Maternal, Child, and Emergency Referral Policy
Health Insurance, Cash Barriers, and Household Protection
Governance, Data, and Public Accountability at LGA Level
Policy Model and Local Government Readiness Formula
Implementation Roadmap for Rural Health Renewal
Conclusion: Making Local Health Governance Visible
List of Tables and Figures
Table 1. Local-government rural health-policy compact for Kevin I. Onyeberechi
Table 2. Rural healthcare risk and policy response matrix for Kevin I. Onyeberechi
Figure 1. Rural service-pressure profile.
Figure 2. BHCPF statutory funding logic.
Figure 3. Rural maternal care policy priorities.
Figure 4. Local government rural-health policy package.
Figure 5. Implementation sequence score.
Chapter 1: Introduction: Rural Policy at the Point of Care
1.1 Rural health policy must be judged where care is needed
Rural health policy begins in the ordinary places where Nigerians seek help: the primary health centre, the maternity room, the drug shelf, the referral vehicle, and the household that must decide whether care can be afforded. A reform that does not change those places has not yet reached the people it claims to serve.
Nigeria’s policy commitments on health insurance and primary care are important, but they need local proof. The practical question is whether a local government can make a facility open reliably, keep workers present, support referral, protect households from cash pressure, and maintain records that can be checked. (Federal Republic of Nigeria, 2022)
Kevin I. Onyeberechi’s central concern is service credibility. The paper treats policy as a duty to organize people, money, supplies, data, and authority so that rural residents receive care early enough and with enough dignity to trust the system.
1.2 Evidence, context, and professional judgement
Evidence on rural health must be read close to the community. A national indicator may show a financing gap or service weakness, but it does not explain the road condition, market-day movement, informal payment practice, staff absence, or family fear that shapes care-seeking in a particular local government.
The stronger academic posture is careful judgement. Where figures are incomplete, the answer is not forced certainty; it is a monitoring plan that combines facility review, community feedback, household cost tracking, and service data. UHC monitoring reinforces the need to connect financial protection with real access. (World Health Organization & World Bank, 2025)
This study uses evidence as a management instrument. Reports and laws matter because they help identify weak links: which households remain uncovered, which facilities lack readiness, which referral routes fail, and which authority should act before the next avoidable harm.
1.3 Management choices that decide outcomes
Rural outcomes are often decided by the small mechanics of management. A register that is not updated, a claims file that is delayed, a staff roster that is ignored, or a referral note that is not followed can undo the value of a national policy.
Local government health leadership must know more than totals. It should know which facilities are actually delivering care, which communities stay away, which workers need support, and which services are blocked by cost or distance.
Policy becomes credible when it alters the experience of care. Enrolment, funding, outreach, and committees should be judged by whether they reduce delay, protect the household, improve attendance, strengthen referral, and create answerability.
1.4 Risks, trade-offs, and safeguards
Rural reform carries familiar risks: funds can be delayed or misused, insurance can become paper coverage, committees can be captured, and workers can be posted to unsafe or unsupported environments. Naming these risks is part of serious policy work.
The safeguards should be visible and practical. Funding records, facility readiness checks, staff attendance, community complaints, and referral outcomes must be traceable enough for leaders and communities to know what changed.
A rural health policy that cannot be audited will eventually become another promise. The standard in this paper is simple: policy should be close to the patient, clear in responsibility, and honest about the work still unfinished.
Figure 1. Rural service-pressure profile.
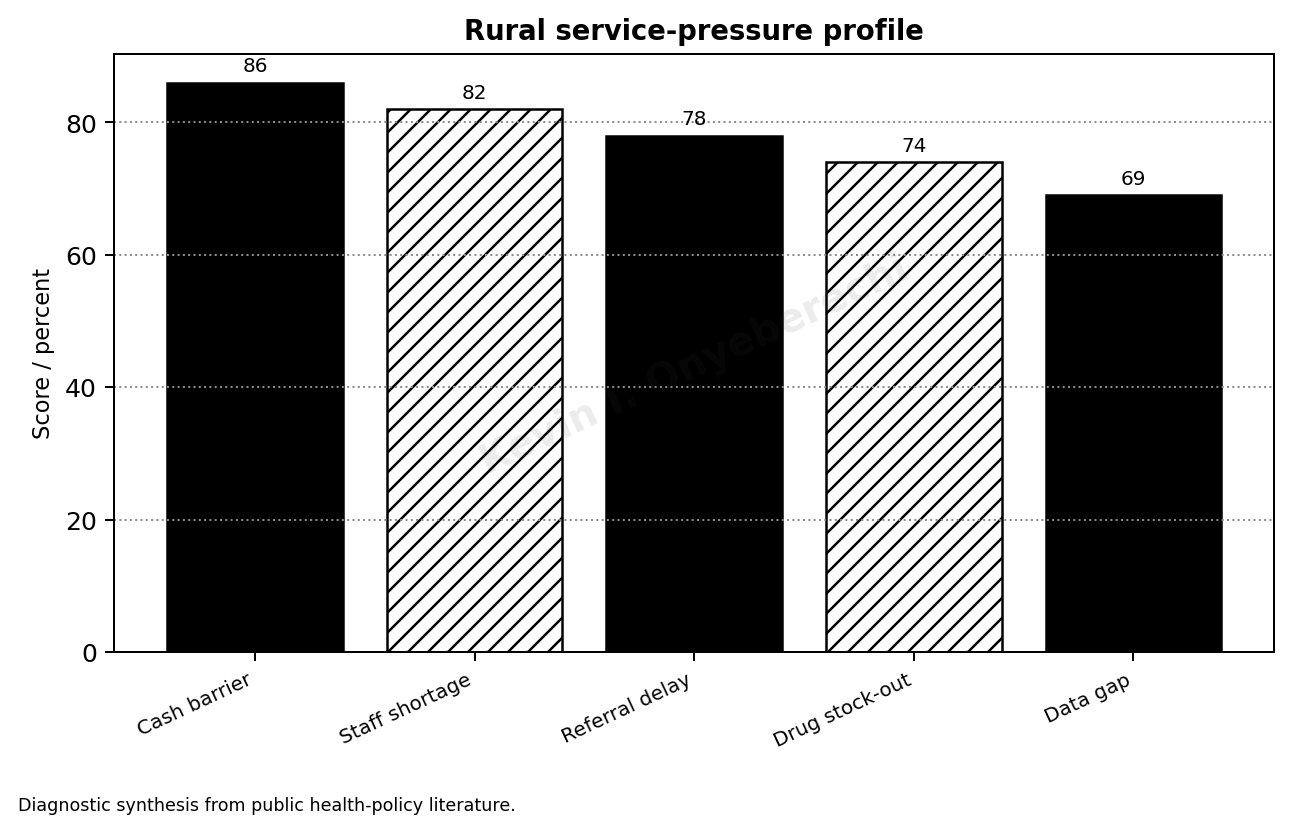
Source: Diagnostic synthesis from public health-policy literature.
Chapter 2: Nigeria’s Rural Health Burden and Local Government Responsibility
2.1 Rural health burden and uneven access
Nigeria’s rural health burden is shaped by distance, poverty, weak infrastructure, and uneven service capacity. Many families delay care because the journey, the expected payment, and the memory of past disappointment make early treatment difficult.
Demographic and health evidence shows why rural planning cannot depend on national averages alone. Maternal and child outcomes, skilled care, immunization, and access to routine services often vary by place, wealth, and education. (National Population Commission & ICF, 2025)
The local government area is close enough to see these differences before they become tragedy. It can identify the communities missing outreach, the facilities with weak staffing, and the referral routes that fail when pressure rises.
2.2 What rural households experience
A rural household experiences the health system as a chain of decisions. The family may choose between waiting, borrowing, buying medicine nearby, travelling to a facility, or returning home when the cost becomes impossible.
Those choices are policy evidence. When formal care is too expensive, too far, or too uncertain, people do not simply ignore healthcare; they manage risk with the options available to them. World Bank health-financing data make the cash burden especially important to any serious rural analysis. (World Bank, 2026)
The paper reads access through dignity as well as distance. A facility that is near but disrespectful, understocked, or unpredictable may still be avoided. Trust is therefore a service condition, not a public-relations slogan.
2.3 Local government responsibility and authority
Local government health responsibility often sits between public expectation and limited control. Communities expect visible service, while major decisions on staffing, funding, procurement, and insurance may involve state or federal systems.
That complexity should not become an excuse for silence. Local authorities can still supervise facilities, review service data, support community engagement, document gaps, and escalate failures with evidence.
The management task is to clarify what can be corrected locally and what must be demanded from higher authority. Rural health governance improves when limits are named instead of hidden.
2.4 The danger of average-based policy
Average-based reporting can make the weakest rural areas disappear. A state may report progress while difficult communities remain outside effective service. A facility may submit numbers while the poorest households still cannot use the care.
Local review should separate data by place, service type, poverty, gender, and facility readiness. A local government that can see its weakest points can direct supervision and resources with greater honesty.
The safeguard is evidence that names the problem. General progress is not enough when one community still has no reliable maternal referral or one facility repeatedly runs without essential supplies.
Figure 2. BHCPF statutory funding logic.
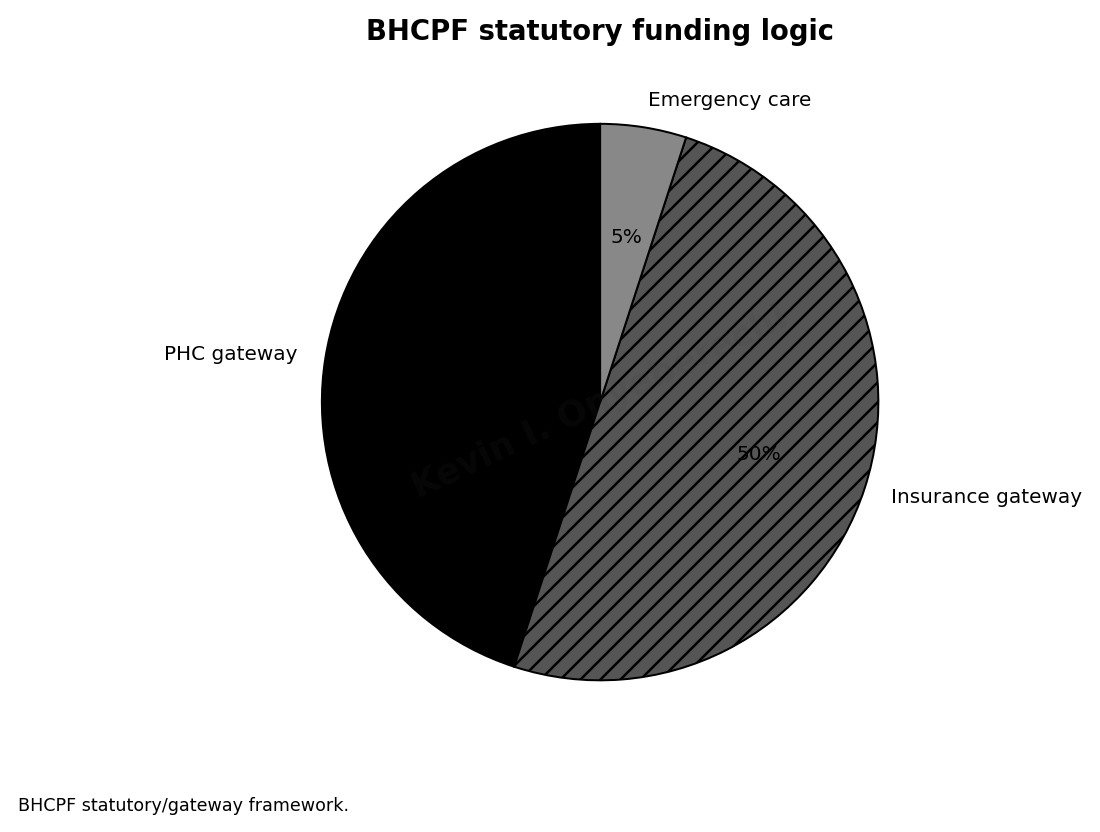
Source: BHCPF statutory/gateway model.
Chapter 3: Primary Health Care Funding and the BHCPF Pathway
3.1 BHCPF as a test of primary care seriousness
The Basic Health Care Provision Fund is important because primary health care cannot survive on aspiration alone. Rural facilities need predictable support for consumables, minor repairs, basic equipment, outreach, records, and routine operations.
Recent BHCPF reform language places useful attention on facility-level funding and accountability. The rural test is whether support arrives in a form that changes readiness, not whether disbursement can be announced. (Federal Ministry of Health and Social Welfare, 2025; National Primary Health Care Development Agency, 2026)
Funding should be tied to visible service improvement: longer reliable service hours, fewer stock-outs, cleaner records, functioning equipment, and stronger referral coordination.
3.2 Facility funding and the credibility of service
Facility funding can reduce delay because it gives local teams a way to respond to practical barriers before they grow into service failure. A missing form, a broken delivery light, or a minor repair can damage care when every response depends on distant approval.
Money alone will not solve the problem. Staff and community representatives should understand how facility funds are approved, what they are used for, and which service gap each expenditure addresses.
The best spending decisions are made from the service floor. Workers who see stock-outs, broken equipment, and referral delays should have a route for turning that knowledge into action.
3.3 Accountability in the funding pathway
Accountability in the funding pathway should follow every naira from allocation to service effect. A facility should know what it received, what was bought, who verified delivery, and what problem the purchase was meant to solve.
Local health authorities should read expenditure beside service data. If antenatal care remains weak, if stock-outs persist, or if referral completion does not improve, the spending pattern deserves review.
Good records also protect honest workers. They show what was requested, what arrived, what did not arrive, and which level of authority has failed to respond.
3.4 Safeguards for rural primary care funding
Primary care funding can be captured by weak documentation, local politics, and spending that satisfies paperwork rather than patients. Rural communities often lack the power to challenge misuse unless information is made visible.
A simple facility finance display can help: allocation received, use approved, date spent, item delivered, service gap addressed, and date for next review. The device is modest, but its discipline is powerful.
Funding should never be presented as success by itself. The success lies in safer delivery, better attendance, essential supplies, stronger outreach, and fewer families turned back by avoidable failure.
Figure 3. Rural maternal care policy priorities.
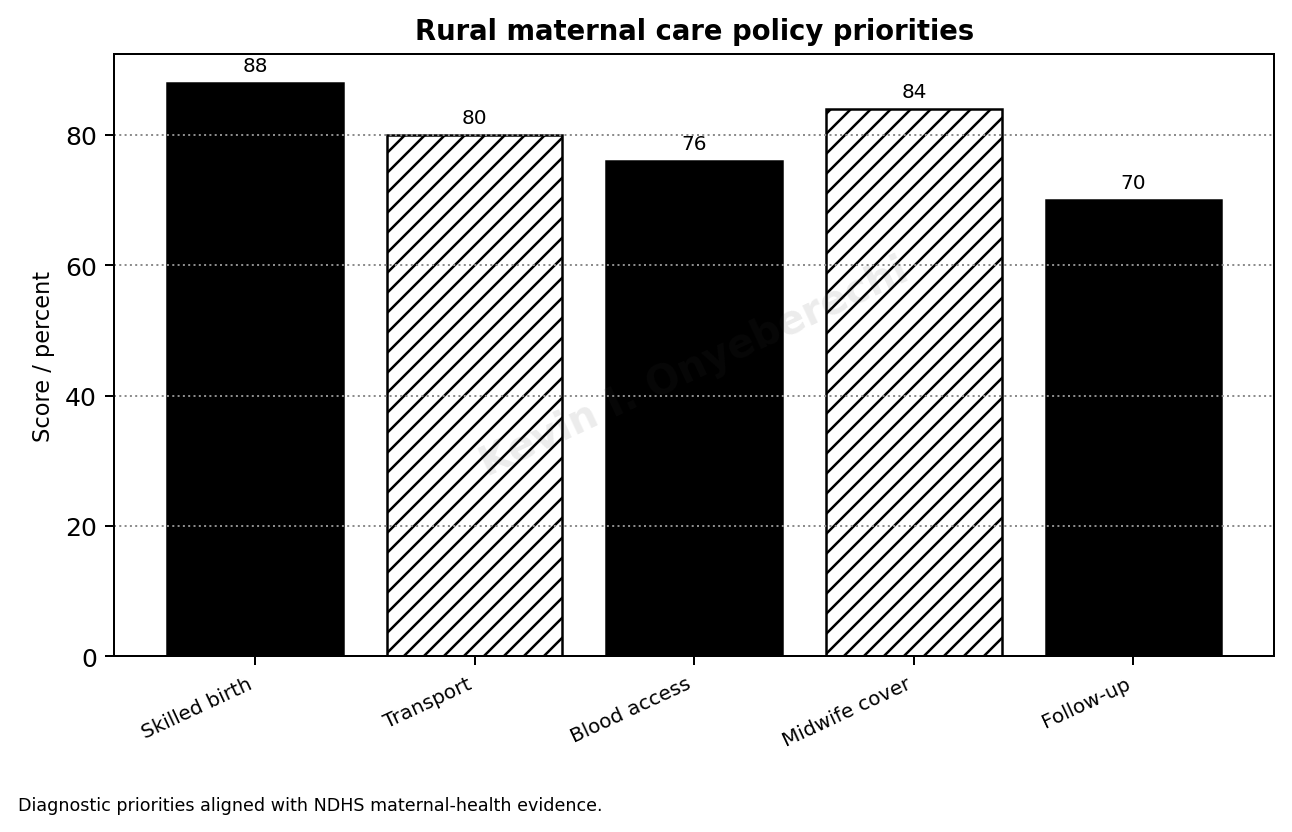
Source: Diagnostic priorities aligned with NDHS maternal-health evidence.
Read also: Managed Care Models In Healthcare By Cynthia Anyanwu
Chapter 4: Rural Workforce, Community Health Workers, and Retention
4.1 Workforce retention as rural patient protection
The rural health workforce is the living capacity of the system. Nurses, midwives, community health workers, and supervisors detect danger, sustain routine care, educate households, and hold the line between public policy and lived experience.
Workforce shortages have global dimensions, yet rural Nigeria feels the pressure with special sharpness. When a rural facility loses experienced staff, communities may lose the only dependable point of care within reach. (World Health Organization, 2025)
Retention is therefore patient protection. Pay matters, but rural workers also need housing, safety, equipment, supervision, career routes, and respect for the difficulty of their service.
4.2 Community health workers and local trust
Community health workers bring local knowledge that no distant office can manufacture. They understand language, settlement patterns, family concerns, seasonal movement, and the fears that keep people away from formal care.
Local trust should still be matched with clinical discipline. Community closeness does not remove the need for training, supervision, supplies, and clear referral. Workers should not be asked to carry professional risk without institutional support.
Their strongest value appears when local knowledge is connected to a supervised care team. Outreach, immunization tracing, maternal follow-up, health education, and complaint reporting all improve when community workers are properly supported.
4.3 Supervision that improves practice
Supervision should improve practice, not simply record that a visit occurred. A useful visit checks attendance, stock, infection prevention, records, referral notes, complaints, and worker concerns.
Poor supervision teaches workers that reporting problems changes nothing. It also teaches communities that complaints have no effect. That silence can become dangerous.
Supervisors need preparation and authority. They should arrive with prior data, compare it with what they see, agree on action, and escalate problems beyond facility control.
4.4 Workforce dignity and accountability
Workforce dignity and accountability must stand together. Unsafe conditions should not be ignored, but neither should absenteeism, poor records, or disrespectful care.
A rural workforce compact should be explicit. Workers owe attendance, respectful service, accurate records, and outreach participation. Local authorities owe supervision, equipment, safety support, fair communication, and a route for grievances.
Balanced evidence protects both sides. Attendance, complaints, service volume, stock reports, and worker feedback should be read together so that blame does not replace understanding.
Figure 4. Local government rural-health policy package.
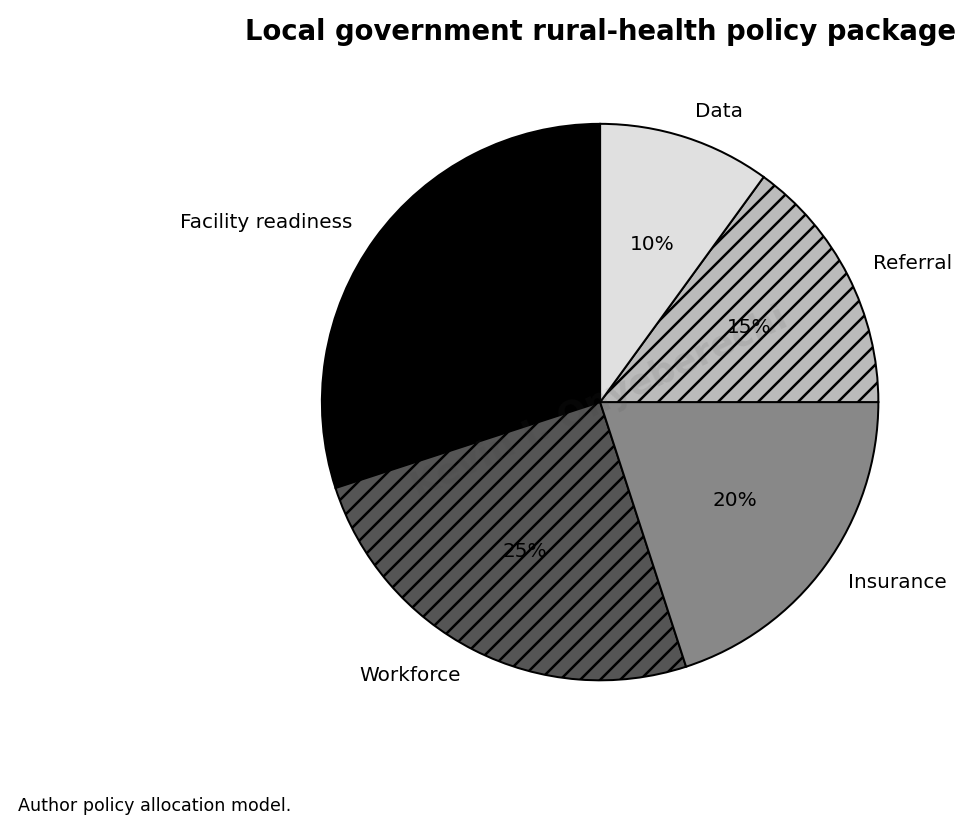
Source: Author policy allocation model.
Table 1. Local-government rural health-policy compact for Kevin I. Onyeberechi
| Policy area | LGA-level action | Evidence of progress |
| PHC funding | Publish facility receipts and spending lines | Monthly facility funding register |
| Workforce | Retain rural nurses and CHWs with hardship support | Vacancy and attendance dashboard |
| Referral | Create ward-to-facility transport plan | Referral completion rate |
| Insurance | Enroll poor and informal households | Utilisation without cash delay |
| Data | Use registers for decisions, not only reporting | Quarterly community review |
Note. Table prepared for Kevin I. Onyeberechi; black-and-white NYCAR publication format.
Chapter 5: Maternal, Child, and Emergency Referral Policy
5.1 Maternal and child health as a rural governance test
Maternal and child health show whether rural governance can respond on time. Pregnancy, birth, newborn care, immunization, nutrition, and malaria treatment all depend on timing and trust.
Nigeria’s demographic and health data keep maternal and child services at the centre of any rural policy discussion. Skilled care and follow-up are not administrative categories; they are survival pathways. (National Population Commission & ICF, 2025)
Planning should begin with the woman’s journey. Distance, transport cost, night referral, skilled-worker presence, and benefit coverage determine whether policy reaches the body in time.
5.2 Referral readiness and emergency time
Referral should be treated as a completed pathway, not advice. A facility that tells a patient to go elsewhere has not finished its duty if transport, records, communication, and receiving care remain uncertain.
Emergency time is unforgiving. Bleeding, sepsis, convulsion, severe malaria, labour complications, and newborn danger signs cannot wait for ordinary bureaucratic pace.
The realistic goal is not to put a full hospital in every settlement. The goal is to ensure that primary care recognizes danger early, referral routes are known, and receiving facilities are prepared.
5.3 Practical controls for maternal and child services
Local governments need practical controls for maternal and child services: antenatal registers, delivery tracking, emergency contact lists, newborn follow-up, immunization defaulter tracing, and review of maternal deaths where they occur.
A rural facility should know which pregnant women missed visits, which children missed immunization, which communities present late, and which referrals did not reach the next level of care.
Health education must remove fear rather than blame families. Communities delay for reasons rooted in cost, distance, and experience; policy must respond to those reasons honestly.
5.4 Safeguarding dignity in maternal and child policy
Maternal and child policy can fail through disrespect even when the technical service exists. A woman who is insulted, overcharged, ignored, or humiliated may warn others away from the facility.
Safeguards should include respectful maternity care, complaint routes, review of informal charges, facility readiness checks, and clear explanation of covered services.
The policy aim is a rural pathway where the mother, newborn, and child are not left to negotiate care alone at the moment of greatest need.
Figure 5. Implementation sequence score.
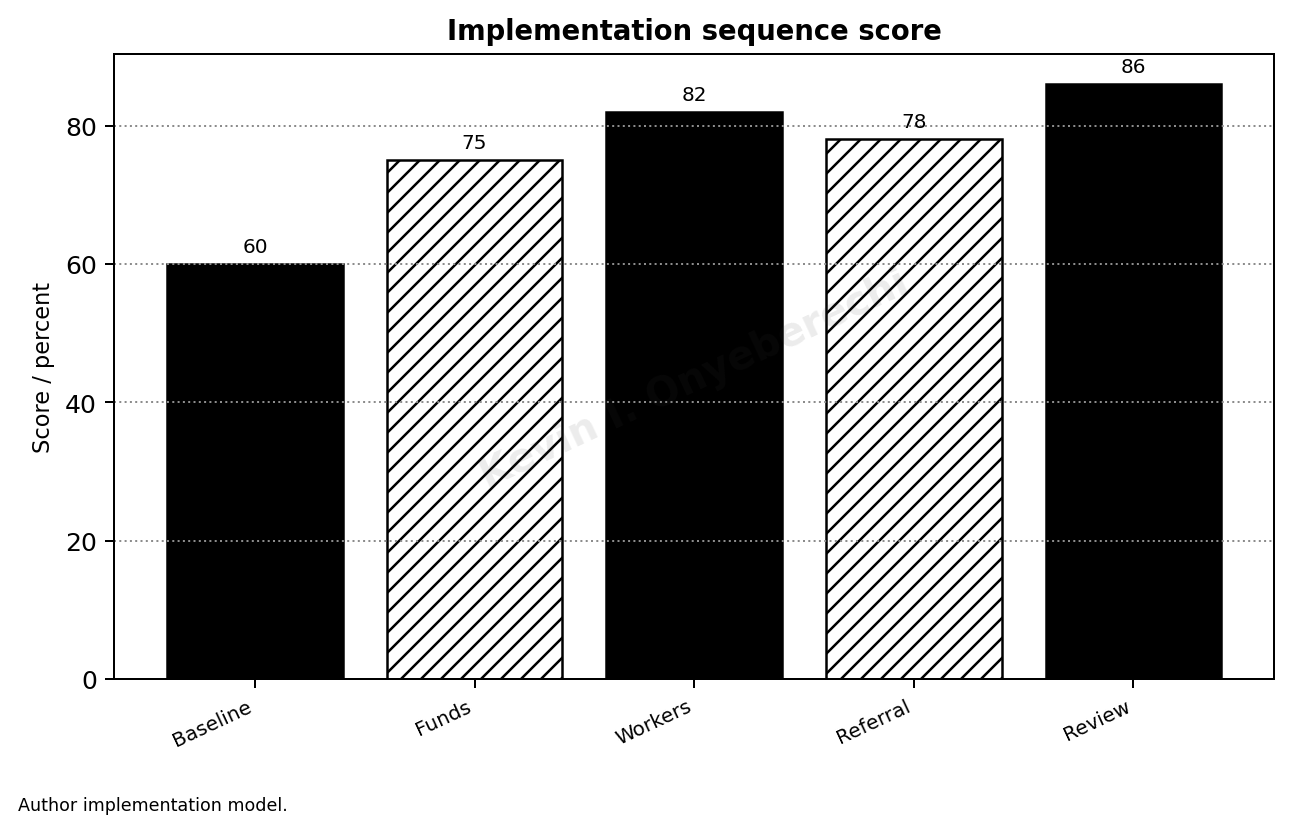
Source: Author implementation model.
Chapter 6: Health Insurance, Cash Barriers, and Household Protection
6.1 Household cost as a barrier to timely care
Household cost remains one of the strongest reasons rural people delay care. Illness competes with food, school fees, transport, farm inputs, and debt; when money is scarce, treatment may wait until risk has grown.
Health-financing indicators and UHC monitoring explain why financial protection must be central to rural policy. A system that depends on cash at the point of care gives poverty too much power over clinical timing. (World Bank, 2026; World Health Organization & World Bank, 2025)
Rural health reform must make formal care easier to seek early. Insurance, public funding, emergency support, and clear benefit rules all matter because they reduce the household’s fear of unaffordable treatment.
6.2 Insurance for informal households
Insurance for informal households must fit irregular income. Farmers, traders, artisans, transport workers, and seasonal labourers do not always have the predictable earnings assumed by formal-sector schemes.
The NHIA Act provides a stronger legal basis for coverage, but local implementation decides whether rural residents believe the promise. A card that does not protect care becomes evidence against the institution. (Federal Republic of Nigeria, 2022)
Enrolment must be tested by what happens after registration: claims acceptance, medicine access, payment delay, provider attitude, and whether households borrow less when illness occurs.
6.3 From enrolment numbers to service protection
Registration figures cannot stand alone. Local governments should know which enrolled households used services, which benefits were denied, which facilities demanded extra payment, and which communities remain outside the scheme.
Facility managers need clear benefit communication. If a service is covered, the patient should not be forced to negotiate. If it is not covered, the explanation should be honest and useful.
Insurance data should be compared with service behavior. Increased antenatal attendance, treatment continuation, and reduced payment delay are stronger signs of protection than enrolment alone.
6.4 Preventing paper protection
Paper protection is the central danger. People may be counted as covered while still facing costs that delay or interrupt treatment.
Safeguards include public benefit lists, claims-payment monitoring, grievance channels, hidden-charge review, and community feedback from those who actually tried to use the scheme.
Financial protection should be judged by family experience: reduced cash demand, fewer interrupted treatments, earlier care-seeking, and stronger maternal and child service use.
Chapter 7: Governance, Data, and Public Accountability at LGA Level
7.1 Governance must be visible at local level
Rural health governance fails when responsibility becomes invisible. A facility may open without medicines, a committee may meet without changing service, and a report may be submitted without producing any decision.
Local government health leadership should make responsibility visible through facility readiness records, worker attendance review, fund tracking, referral monitoring, insurance-complaint analysis, and community feedback.
Governance in this chapter means practical control. It is the ability to know what is happening, decide who must act, check whether action occurred, and explain the result to the community.
7.2 Evidence, context, and professional judgement
Rural health policy must be read from the point where public promise meets ordinary life. A local government plan may look convincing on paper and still fail the woman who travels far for antenatal care, the older patient who cannot afford medicine, or the nurse expected to cover too much work with too little support. (World Bank, 2026)
The evidence points to a chain of conditions rather than a single cure. Financing matters, but money alone does not repair weak supervision. Recruitment matters, but posting staff without housing, security, equipment, and professional support only moves the problem from one office to another.
Professional judgement is needed because rural reform sits inside distance, poverty, local politics, weak infrastructure, staff fatigue, informal payments, poor referral systems, and public distrust created by earlier disappointment.
7.3 Management choices that decide outcomes
The outcomes of rural health policy are often decided by management choices that appear small until they fail. A drug register not updated, a referral note not followed, a late claims payment, or a committee meeting without evidence can undo the promise of reform.
Local government health leadership should treat rural care as a reliability problem. That means knowing which facilities are open, which workers are present, which services are delivered, which households are excluded by cost, and which referral routes are failing.
Health insurance enrolment for rural and informal households should be treated as a management test. The relevant question is whether enrolment changes payment delay, maternal care, medicine access, provider response, household borrowing, and treatment continuation.
7.4 Data, trade-offs, and public safeguards
Data can become a display tool if leaders collect it only to protect the image of performance. Rural health records should protect truth, not reputation.
A useful local data system should track facility readiness, maternal and child services, referral completion, essential medicines, worker presence, insurance problems, and complaints.
Public accountability requires more than internal review. Communities should know where to raise concerns, how complaints are handled, and what actions follow.
Chapter 8: Policy Model and Local Government Readiness Formula
8.1 Why a readiness formula is useful
A readiness formula helps leaders see whether rural services are prepared for the population they claim to cover. Access language alone cannot show whether workers, supplies, referral, finance, and records are working together.
The proposed Local Government Rural Health Readiness Function brings together workforce presence, supply readiness, financing, referral completion, insurance protection, data quality, community trust, and management response.
The model is a management aid, not an official index. It helps local leaders decide whether the next correction belongs in staffing, funding, insurance, referral, records, or community engagement.
8.2 Variables and scoring logic
The model uses normalized scores so that unlike service conditions can be discussed together without pretending they are identical. Each variable should be scored from evidence rather than impression.
One local government may find that referral completion is weaker than funding. Another may discover that enrolment is high while medicine access remains poor.
The value of the formula is discipline. It prevents one preferred intervention from being treated as the answer to every rural health problem.
8.3 How local leaders should use the model
Local leaders should use the model in review meetings with facility officers, finance staff, insurance desk officers, and community representatives. The meeting should end with action, not appreciation speeches.
Comparison across facilities can identify useful practice. A better-performing rural facility may reveal stronger supervision, clearer fund use, active community oversight, or a more reliable referral habit.
The score should trigger thresholds: urgent supervision for very weak readiness, targeted support for moderate weakness, and sustainability review where performance appears stronger.
8.4 Limits of scoring and the need for judgement
Scoring can mislead when the underlying data are weak. A facility may report supplies that are unusable, attendance that does not match service, or committee activity that produces no correction.
The readiness model should therefore be used with field verification, worker testimony, patient complaints, and community feedback.
Numbers should sharpen judgement, not replace it. The patient’s experience remains the final test of whether rural policy is working.
Table 2. Rural healthcare risk and policy response matrix for Kevin I. Onyeberechi
| Risk | Likely effect | Policy response |
| Unfunded PHC | Stock-outs and informal fees | Direct facility financing with audit |
| Worker fatigue | Unsafe workload | Rural retention compact |
| Distance | Late presentation | Transport voucher and referral line |
| Cash payment | Treatment interruption | State insurance and exemption fund |
| Weak data | Blind planning | LGA health intelligence cell |
Note. Table prepared for Kevin I. Onyeberechi; black-and-white NYCAR publication format.
Chapter 9: Implementation Roadmap for Rural Health Renewal
9.1 Implementation must begin with visible service gaps
Implementation should begin with service gaps that rural people already recognize: absent workers, stock-outs, late referral, hidden charges, weak outreach, and complaint routes that lead nowhere.
Local governments should not launch more initiatives than the system can absorb. A credible roadmap selects damaging gaps, assigns responsibility, corrects practical barriers, and checks whether the change reaches households.
The aim is visible improvement. People should see more reliable opening hours, better medicine availability, clearer referral, and a response when they complain.
9.2 Building a practical local roadmap
A practical roadmap should combine facility audit, workforce review, finance tracking, insurance monitoring, referral mapping, community feedback, and leadership review.
Local variation matters. A riverine settlement, a farming community, a peri-urban fringe, and a remote village may need different delivery arrangements while still meeting the same standard of accountability.
Pacing is part of judgement. Stock-outs and unsafe referral delay require quick action, while workforce retention and insurance trust require sustained management.
9.3 Assigning responsibility without hiding behind committees
Implementation weakens when every task is given to a committee and no person has authority to act. Committees may coordinate, but named owners must still carry responsibility.
Review meetings should ask what changed, what persisted, what decision is needed, who owns it, and when the result will be checked.
Complaints from rural communities should be treated as early warnings. Reports of missing drugs, informal fees, absenteeism, or rude treatment give the system a chance to correct itself before trust collapses.
9.4 Keeping implementation honest
The main implementation risk is a clean report covering a weak facility. Paper can move even when care does not.
Political pressure can also distort local health decisions. Resource allocation should be defendable through evidence, not personal loyalty or local influence.
Regular public explanation helps keep reform honest. Communities deserve to know what is improving, what remains difficult, and when the next review will occur.
Chapter 10: Conclusion: Making Local Health Governance Visible
10.1 What rural health renewal should mean
Rural health renewal should mean that people outside urban advantage can reach competent, affordable, respectful care without being punished by geography or poverty.
The paper has argued that national laws and funding pathways are necessary but incomplete. The rural family experiences policy through the local facility, not through the document that announced it.
Kevin I. Onyeberechi’s contribution is practical and grounded: rural health is a matter of public management, institutional dignity, and measurable responsibility.
10.2 What the evidence demands from leaders
The evidence demands service control. Funds must reach facilities, workers must remain in post, insurance must protect households, referral must complete care, and data must lead to correction.
Local governments may not control every funding or staffing decision, but they can still document gaps, supervise facilities, hear complaints, monitor referral, and report failures upward with evidence.
Ambition without delivery discipline becomes another disappointment. Rural communities need reform that can be seen in ordinary care.
10.3 The management standard for local government health policy
The management standard offered by this paper is readiness, protection, and accountability. Readiness asks whether the facility can deliver. Protection asks whether the household can seek care without destructive cost. Accountability asks whether responsibility can be located when service fails.
That standard can guide facility review, budget planning, workforce support, insurance monitoring, referral mapping, and community engagement.
The measure of success is the experience of the person who arrives tired, anxious, and in need of care that should not require begging.
10.4 Final position
Rural health policy in Nigeria will become credible through daily service reliability: open facilities, supported workers, traceable funds, available medicines, completed referral, and protection from cash shocks.
The local government area is close enough to see failure and important enough to organize response when authority, evidence, and accountability are strengthened.
The final position is direct. Rural communities deserve policy that reaches them as care. Anything less is administration without justice.
References
Agency for Healthcare Research and Quality. (2023). TeamSTEPPS 3.0. U.S. Department of Health and Human Services. https://www.ahrq.gov/teamstepps-program/index.html
Federal Ministry of Health and Social Welfare. (2025). FG approves N32.9bn disbursement, unveils BHCPF 2.0 to strengthen primary healthcare accountability. https://health.gov.ng/
Federal Republic of Nigeria. (2022). National Health Insurance Authority Act, 2022. Government Printer.
National Population Commission & ICF. (2025). Nigeria Demographic and Health Survey 2023-24: Key indicators report. DHS Program. https://dhsprogram.com/
National Primary Health Care Development Agency. (2026). Basic Health Care Provision Fund. https://nphcda.gov.ng/bhcpf/
World Bank. (2026). World Development Indicators: Nigeria health expenditure. https://data.worldbank.org/
World Health Organization & World Bank. (2025). Tracking universal health coverage: 2025 global monitoring report. https://www.who.int/publications/i/item/9789240117808
World Health Organization. (2025). State of the world’s nursing 2025. https://www.who.int/publications/i/item/9789240110236