

New York Center for Advanced Research (NYCAR)
A Paige AI Prostate Pathology Case Study in AI-Assisted Cancer Diagnosis
Master’s Research Publication
Research Publication by Ogochukwu I. Okoye
Publication No.: NYCAR-TTR-2026-RP023
DOI: https://doi.org/10.5281/zenodo.20435017
June 2026
Peer Review Statement: This research publication has been reviewed under NYCAR’s internal editorial framework and The Thinkers’ Review. The review assessed master’s-level coherence, source integrity, method suitability, quantitative reasoning, APA 7 alignment, and professional relevance. The work is approved for NYCAR institutional publication.
Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved. NYCAR.
Abstract
Pathology is where many cancer decisions become definite enough for treatment, yet the work is usually invisible to the patient whose future turns on the slide. A prostate biopsy is not just tissue on glass. It is a chain of sampling, fixation, staining, scanning, viewing, interpretation, reporting, communication, and clinical action. Digital pathology changes that chain. Artificial intelligence changes it further, not by removing the pathologist, but by altering what can be highlighted, checked, routed, timed, and audited before a report reaches the treating team.
This master’s research publication examines Paige Prostate as a case in diagnostic safety and workforce sustainability. The device received FDA De Novo authorization in 2021 as software intended to assist pathologists in detecting foci suspicious for cancer during review of digitized prostate biopsy images. That authorization matters, but it is not the whole clinical story. A laboratory still can validate scanners and displays, protect image quality, train users, preserve diagnostic authority, maintain cybersecurity, monitor discrepancy patterns, and decide how algorithmic assistance fits into the practical rhythm of work.
The study uses public regulatory evidence, College of American Pathologists guidance on whole-slide imaging validation, digital pathology literature, and applied management modeling. Its diagnostic-load balance model examines whether validated infrastructure, assistive review, workflow efficiency, and workforce flexibility are sufficient to justify implementation burden and error risk. The model is not presented as hidden clinical data. It is a transparent planning tool for laboratories, health-system leaders, and clinical governance boards.
The argument is deliberately cautious. AI-assisted pathology can help draw attention to suspicious tissue, support consultation, and ease pressure on scarce expertise. It can introduce new risk if it is purchased faster than the laboratory can govern it. Paige Prostate is therefore best understood as a test of clinical stewardship: the technology becomes valuable only when pathologists remain accountable, local validation is serious, monitoring continues after launch, and diagnostic judgment is strengthened rather than displaced.
Keywords: digital pathology; artificial intelligence; Paige Prostate; prostate cancer; diagnostic safety; pathology workforce; whole-slide imaging; clinical AI governance
Contents
Chapter 1: Introduction and Diagnostic Problem
1.1 Why digital pathology matters for diagnostic safety
Cancer diagnosis depends on many hands before a patient hears the word that changes the rest of the consultation. A biopsy is taken, prepared, stained, tracked, reviewed, reported, and translated into treatment. Patients often imagine diagnosis as one decisive moment under a microscope. In reality, diagnosis is a pathway. Each part of that pathway can protect the patient or expose the patient to delay, ambiguity, or error. Digital pathology enters this pathway at a sensitive point because it changes how slides are captured, viewed, shared, stored, and reviewed.
Whole-slide imaging allows tissue sections to be scanned into digital images that can be viewed on a screen rather than through a conventional microscope. The change appears technical, but it has management consequences. Images are captured with sufficient quality. Displays are fit for diagnostic use. File storage and network speed affect the working day. Remote consultation becomes easier, but cybersecurity and access control become more important. Validation moves from a narrow laboratory exercise to a safety condition for the whole service (Evans et al., 2022; Pantanowitz et al., 2013).
In prostate pathology, the stakes are specific. Small foci of carcinoma may carry serious clinical consequences. A pathologist may review a large number of benign cores before finding a small suspicious area. A tool that highlights potentially suspicious regions can support attention, but the clinical duty remains with the pathologist. The managerial question is therefore not whether a machine can point to a region of interest. It is whether the laboratory can introduce that support without weakening responsibility, increasing friction, or creating blind trust in a software output.
1.2 Paige Prostate as a case
Paige Prostate is useful as a case because it is not an abstract prediction about AI in medicine. The FDA De Novo decision identified it as a software-only device intended to assist pathologists in detecting foci suspicious for cancer during review of digitized prostate biopsy images (U.S. Food and Drug Administration, 2021). That intended use is narrow enough to study carefully. The device does not diagnose cancer for the pathologist, sign out reports, or replace histological judgment. It operates inside a workflow where professional responsibility remains visible.
This case avoids a common weakness in AI writing: treating authorization as if it were the same as clinical readiness. Regulatory clearance can show that evidence satisfied a defined review pathway. It does not prove that every laboratory has adequate scanner validation, image management, display quality, network performance, cybersecurity discipline, staff training, quality monitoring, or audit capacity. Paige Prostate therefore makes the distinction between device authorization and local clinical governance impossible to ignore.
The study frames the case through three concerns. The opening point is diagnostic safety: can assistive software reduce the risk that suspicious tissue is missed while preserving pathologist judgment? The next point is service management: can the tool fit into the day-to-day laboratory without creating hidden delays or burdens? The final point is workforce sustainability: can digital systems support scarce diagnostic expertise without pretending that expertise is optional? These concerns are connected, because a system that helps diagnosis but exhausts the service will not remain safe for long.
1.3 Research aim and questions
The aim of this publication is to examine how AI-assisted digital pathology can be governed as a patient-safety and workforce-management intervention. The focus is Paige Prostate, but the wider contribution concerns any laboratory considering assistive software in diagnostic work. The question is not simply whether AI performs well in a controlled evaluation. The question is whether the clinical setting can carry AI responsibly.
The research asks four practical questions. What does the Paige Prostate case reveal about the limits of AI-assisted diagnostic support? Which whole-slide imaging and laboratory conditions are required before such support can be trusted in practice? How can diagnostic-load balance be modeled without inventing clinical findings? Which governance routines protect pathologist authority, patient safety, data integrity, and workforce sustainability after implementation?
The paper is written for health-service managers, pathology leaders, clinical governance committees, and graduate researchers who can evaluate medical AI without either fear or excitement taking control of the analysis. It treats AI as a tool inside a service. The service, not the software alone, is the object of management.
Table 1. Digital pathology operating requirements
| Requirement | Management question | Risk if weak |
| Whole-slide imaging | Are scanners validated for intended case types? | Image quality compromises diagnosis. |
| Viewer and display | Can pathologists review safely and efficiently? | Digital review becomes slow or unsafe. |
| AI deployment | Is intended use narrow and understood? | Automation bias or misuse. |
| Cybersecurity | Are images and patient data protected? | Diagnostic and privacy risk. |
| Quality monitoring | Are discrepancies tracked after launch? | Silent performance drift. |
Note. Original table prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye.
Chapter 2: Digital Pathology and AI Literature
2.1 Whole-slide imaging as a clinical platform
Digital pathology is often introduced as a matter of scanning slides, but that description understates the change. Whole-slide imaging turns diagnostic tissue into a digital object that can be viewed, stored, transmitted, measured, and analyzed through software. The slide is still rooted in histological preparation, but its use now depends on scanner performance, image compression, viewer design, display calibration, bandwidth, data storage, and clinical acceptance. Every one of those elements can affect diagnostic confidence.
The College of American Pathologists guideline work on whole-slide imaging validation is central because it insists that laboratories validate their own systems before diagnostic use. Validation is not ceremony. It asks whether the digital system can produce interpretations equivalent to established practice for the intended use, case mix, scanners, displays, and users (Evans et al., 2022; Pantanowitz et al., 2013). A digital pathology program that skips or trivializes validation is not modern. It is under-governed.
The literature shows that digital pathology is an infrastructure change. Scanners can fail, images can be incomplete, focus can be poor, and file access can be slow. A pathologist may spend less time at the microscope but more time managing image navigation if the viewer is poorly designed. Laboratory leaders therefore can examine digital pathology as work design, not just image acquisition. A system that looks efficient in a vendor demonstration may feel different during a high-volume diagnostic session.
2.2 AI assistance and the pathologist’s role
AI in pathology is best understood as assistive decision support rather than independent clinical authority. The distinction is not cosmetic. Pathologists integrate morphology, clinical history, specimen context, staining quality, differential diagnosis, and local reporting standards. Software may identify a suspicious region or provide a probability signal, but it does not carry the professional obligations that belong to a registered clinician. The College of American Pathologists has framed this point in plain terms: AI tools may make predictions, while pathologists make diagnoses (College of American Pathologists, 2025). This distinction aligns with broader diagnostic-pathology literature that treats AI as support for professional interpretation rather than a replacement for pathologists (Shafi & Parwani, 2023).
Diagnostic AI literature supports interest but not complacency. Reviews of AI in digital pathology show promise across several applications, yet they describe variation in study design, data composition, external validation, and risk of bias (McGenity et al., 2024). The practical lesson is not that AI lacks value. It is that the value depends on context, evidence quality, clinical fit, and post-deployment review. A laboratory cannot rely on a headline accuracy figure without asking where the data came from and whether the local setting resembles the evaluated setting.
The risk of automation bias deserves attention. A pathologist may place too much trust in an algorithmic highlight, especially under time pressure. The opposite risk is possible: a user may ignore a useful alert because the system is poorly introduced, poorly explained, or experienced as an intrusion. Training can address both tendencies. Human oversight is not preserved by writing it into a policy; it is preserved through workflow, culture, time, and audit.
2.3 Workforce pressure and diagnostic demand
Pathology services face a difficult workforce problem. Cancer services require timely diagnosis, reporting standards are demanding, and subspecialty expertise is unevenly distributed. Digital pathology can support remote review, consultation, and workload sharing. AI may help triage attention or reduce avoidable delay in defined tasks. Those possibilities are significant, but they do not remove the need for trained pathologists. In fact, new digital systems require pathologists to learn additional review practices, supervise validation, participate in governance, and interpret new kinds of evidence.
Workforce sustainability therefore belongs within more than productivity. A laboratory may introduce AI to save time, but early implementation can increase workload through validation, training, troubleshooting, quality review, and user support. The burden may be justified if it produces safer, more flexible service over time. It becomes damaging when the business case counts future efficiency while ignoring the transition work required to get there.
The better workforce question is whether digital pathology allows scarce expertise to be used more wisely. Can high-risk cases be flagged earlier? Can remote consultation reduce bottlenecks? Can less experienced staff gain support without losing supervision? Can routine review become more organized while complex interpretation remains protected? Those are management questions, not software features.
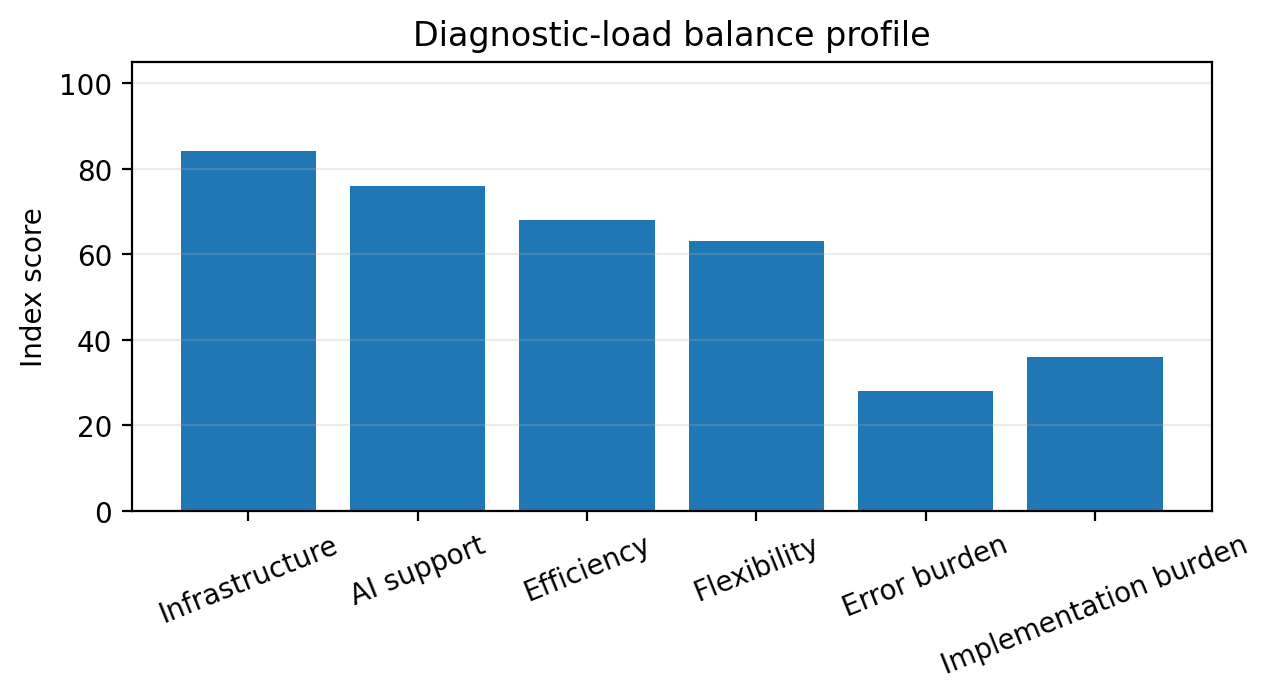
Figure 1. Author-developed visual prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved.
Chapter 3: Regulatory and Case Context
3.1 The FDA De Novo authorization
The FDA De Novo decision for Paige Prostate provides the regulatory anchor for this study. Public FDA material states that Paige Prostate is software intended to assist pathologists in detecting foci suspicious for cancer during review of digitized prostate biopsy images (U.S. Food and Drug Administration, 2021). That wording matters. It establishes assistance, suspicion, digitized images, prostate biopsy, and pathologist review as the central boundaries.
A regulatory boundary is a safety boundary. A laboratory that uses a tool outside its intended use invites clinical and legal confusion. A device cleared for assisting with suspicious foci in prostate biopsy review cannot be casually generalized to other cancers, other specimen types, or unsupported diagnostic decisions. Responsible implementation begins with the discipline of intended use.
The public case material is enough to support analysis, but not enough to prove every local outcome. It does not show how each laboratory trains users, handles exceptions, archives image data, monitors false alerts, or reports turnaround changes. That is why this publication separates the regulatory case from the local governance case. FDA authorization can open a path; local validation decides whether that path is safe enough for a given service.
3.2 Evidence boundaries
AI healthcare publications often lose credibility by overstating what a public source can show. A product summary can describe intended use and evidence reviewed for authorization. It cannot prove equity across all populations, user behavior across all laboratories, or sustainability under staffing pressure. That boundary matters in digital pathology because the same software can perform differently when the scanner, case mix, user training, network, or display changes.
The evidence base used here is therefore layered. FDA material supports the Paige Prostate device context. CAP guidance supports the importance of whole-slide imaging validation. Digital pathology literature supports the need for external evaluation and careful clinical adoption. AI governance sources, including the NIST AI Risk Management Framework, support risk identification, measurement, management, and monitoring across the life of an AI system (NIST, 2023).
The study does not claim that private Paige data, local laboratory logs, or patient-level outcomes were analyzed. It provides a management framework that a laboratory could adapt with local data. That restraint is part of the publication standard. A planning model is valuable when it states what it can and cannot prove.
3.3 From authorization to service adoption
The transition from authorized device to service adoption is where many health technologies succeed or fail. The laboratory can identify the intended pathway, determine which cases qualify, train pathologists, set review rules, define escalation, protect data, measure discrepancy, and decide what counts as a failed or concerning use case. No single announcement accomplishes that work.
The case raises responsibility questions. If software highlights a suspicious area and the pathologist disagrees, what record is preserved? If the system misses a focus that the pathologist finds, is that event logged for performance review? If the pathologist misses a focus that the software highlighted, how is that handled in education and quality assurance? These questions are uncomfortable because they connect human judgment with machine assistance. Avoiding them does not make the risk disappear.
Adoption is paced by readiness. A smaller laboratory may need a different rollout than a large academic center. A site with mature digital pathology infrastructure may be able to focus on AI governance. A site still building whole-slide imaging capacity may can solve scanner validation and image-management problems before adding algorithmic support. The tool enters the laboratory as part of a system, not as a standalone answer.
Chapter 4: Workflow, Validation, and Diagnostic Safety
4.1 Workflow fit
Workflow fit is one of the most important safety questions in AI-assisted pathology. A system that interrupts reading, slows case navigation, or produces unclear alerts can weaken service quality even when its technical performance appears attractive. A pathologist reviewing a long list of cases needs the software to integrate with the viewer, the laboratory information system, the reporting routine, and the local sequence of work. Anything else becomes a The next point job.
The workflow question can be tested through observation. How many clicks are required? Where does the alert appear? Does it arrive before, during, or after the pathologist’s review? Can the user move easily between regions? Is the alert explainable enough to prompt examination without creating false authority? Are disagreements recordable? Do case files remain easy to locate after review? These details decide whether the service becomes safer or simply more complicated.
Workflow fit is a matter of attention. AI assistance may be most useful when it helps prevent fatigue-related oversight, particularly in large volumes of benign-appearing tissue. Yet if the tool creates too many signals, pathologists may learn to ignore it. Alert burden is a clinical governance issue. A laboratory can know whether the alert pattern supports careful review or becomes noise.
4.2 Validation before use
Validation is the laboratory’s The opening point serious act of self-protection. CAP guidance on whole-slide imaging emphasizes validation for intended diagnostic use, recognizing that a system’s performance is assessed in the environment where it will be used (Evans et al., 2022; Pantanowitz et al., 2013). AI support adds another layer. The scanner, tissue preparation, image quality, user interface, algorithm, and case mix all interact.
A practical validation plan for Paige Prostate use would include a defined case set, qualified pathologists, scanner and display details, acceptance criteria, discrepancy review, documentation, and governance sign-off. It would not be enough to say that the device has regulatory authorization. Local validation asks a different question: does this site’s digital pathway support safe use for the intended cases and users?
Validation requires negative space. Which cases are excluded? What happens with poor image quality? How are atypical small foci, inflammation, artifacts, or unusual histology handled? What if the tissue preparation does not resemble cases in the original evidence base? A good validation process is not built to confirm confidence. It is built to expose where confidence is too easy.
4.3 Diagnostic safety after launch
Post-launch safety matters because performance is not frozen at go-live. Staff change, scanners are serviced, software versions may change, case mix shifts, workloads fluctuate, and reporting practices develop shortcuts. A laboratory that treats implementation as complete after launch may miss the moment when safe use begins to drift.
Monitoring requires turnaround time, discrepancy review, false alert burden, missed-alert review, user feedback, case routing, image quality, technical downtime, and pathologist confidence. Some measures are numerical; others require professional review. A dashboard can show patterns, but it cannot interpret every pathology disagreement. Governance boards need both metrics and professional discussion.
Diagnostic safety includes the patient’s timeline. An AI-assisted service that improves internal review but delays report release has not clearly helped the patient. Conversely, a tool that reduces delay while preserving review quality may support access to treatment. Managers can connect laboratory metrics to clinical consequences: the report, the multidisciplinary team, the patient consultation, and the treatment plan.
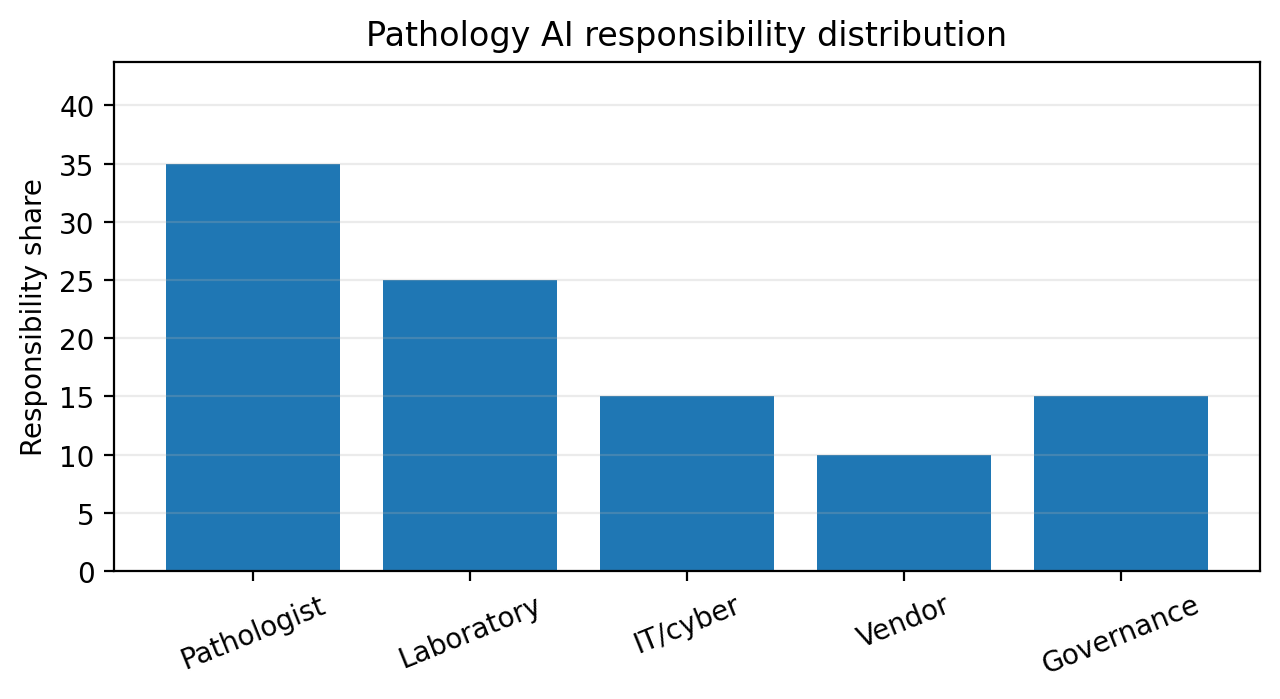
Figure 2. Author-developed visual prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved.
Chapter 5: Workforce Sustainability and Professional Practice
5.1 The pathologist as accountable professional
AI assistance changes the work of the pathologist but does not erase professional accountability. The pathologist still examines the tissue, interprets morphology, considers clinical context, resolves uncertainty, and signs the report. A software output is part of the evidence environment. It is not the clinician.
This distinction protects patients and professionals. Patients are entitled to know that a qualified person remains responsible. Pathologists need organizations that do not pressure them to accept algorithmic suggestions for the sake of speed. Vendors need feedback, but they do not supervise diagnosis. Laboratory leadership can preserve these boundaries in policy, training, and daily work.
Accountability requires time. A pathologist cannot exercise meaningful oversight if workloads are arranged as if algorithmic support has already solved the labor problem. If AI is used to increase volume without preserving review time, diagnostic authority becomes formal rather than practical. Workforce sustainability depends on honest workload planning.
5.2 Training and professional confidence
Training cannot be limited to a demonstration of buttons. Pathologists require an understanding of intended use, evidence limits, alert behavior, disagreement handling, documentation, and local escalation. Laboratory scientists and informatics staff need parallel training around scanning, image quality, data handling, and technical faults. Managers need training in what the tool can and cannot justify.
Professional confidence grows when the system allows users to question it. Pathologists need a pathway for reporting confusing alerts, false positives, suspected misses, and workflow problems. Those reports are reviewed without blame. Early adoption always reveals frictions that were not visible in procurement conversations.
The workforce benefit of digital pathology appears when the technology gives clinicians more usable time, better access to consultation, easier review of difficult cases, and greater flexibility across sites. If the system creates a permanent layer of troubleshooting and administrative work, the promised benefit weakens. This is why training and user feedback belong inside the workforce model rather than outside it.
5.3 Remote work and service resilience
Digital pathology can support remote review and networked expertise. That is valuable for resilience. A service may use digital slides to route cases to subspecialists, support consultation between hospitals, cover short-term absence, or reduce geographic bottlenecks. For regions with uneven pathology capacity, remote review can be more than convenience.
Remote work still requires governance. The display environment, network security, authentication, data storage, reporting interface, and local policy are fit for diagnostic work. A pathologist reviewing at a remote site does not become less accountable, and the laboratory does not become less responsible for the conditions of review. Remote flexibility is safe only when the environment is controlled.
Workforce sustainability therefore involves both distribution and protection. The service can use scarce expertise more flexibly, but it can protect concentration, supervision, and peer contact. The profession cannot be sustained by isolated clinicians working through screens without adequate connection to colleagues, quality review, or service leadership.
Chapter 6: Diagnostic-Load Balance Model
6.1 Purpose of the model
The diagnostic-load balance model is designed for planning, not for claiming hidden empirical findings. It asks whether the burden of implementing AI-assisted digital pathology is justified by the clinical and workforce benefits expected in a defined setting. The model is deliberately transparent, because healthcare managers require tools that can be debated rather than black boxes that imitate certainty.
The model uses six components. Four are potential benefits: validated infrastructure, assistive review value, workflow efficiency, and workforce flexibility. Two are burdens: error risk and implementation burden. The balance is favorable when the benefit components outweigh burden in a way supported by local evidence. The balance is not favorable when the tool adds complexity faster than the laboratory can govern it.
The model can be expressed as DLB = 0.25V + 0.20A + 0.20E + 0.15F – 0.10R – 0.10B. V represents validated infrastructure, A assistive review value, E workflow efficiency, F workforce flexibility, R error risk, and B implementation burden. Scores are normalized on a 0 to 100 scale. The weights are author-developed planning weights, not universal constants.
6.2 Interpreting the components
Validated infrastructure receives the highest weight because an AI tool depends on the digital pathway that carries it. If scanner validation, display conditions, image quality, data storage, and viewer performance are weak, the algorithm enters an unstable environment. No model of diagnostic support can rescue a poorly governed digital foundation.
Assistive review value refers to the capacity of the tool to direct attention in a clinically useful way. It includes whether suspicious regions are highlighted clearly, whether user disagreement is possible, whether alerts support rather than interrupt review, and whether the evidence base fits the intended case type. Workflow efficiency examines whether review, reporting, consultation, and audit become more manageable in practice.
Workforce flexibility captures the ability to route cases, support remote review, or make scarce expertise more accessible. Error risk includes false reassurance, automation bias, poor image quality, missed foci, and overreliance on the tool. Implementation burden includes validation, procurement, training, maintenance, cybersecurity, vendor management, and quality monitoring. A low burden score is not always desirable; it may indicate that the laboratory has not counted the work honestly.
6.3 Example interpretation
In a planning example, a laboratory might score validated infrastructure at 84, assistive review at 76, workflow efficiency at 68, workforce flexibility at 63, error risk at 28, and implementation burden at 36. The weighted result would be DLB = 0.25(84) + 0.20(76) + 0.20(68) + 0.15(63) – 0.10(28) – 0.10(36), which equals 52.85 on the chosen scale. The number is not a claim about Paige Prostate performance. It is a way to ask why the score is not higher and what action would improve readiness.
The model becomes useful when the components lead to decisions. If infrastructure is low, the laboratory invests in scanner validation and image governance before expanding use. If workflow efficiency is low, pathologists and informatics staff review the viewer and reporting interface. If error risk is high, training and discrepancy monitoring intensify. If implementation burden is high but benefits are high, leadership may proceed with a phased launch rather than a broad rollout.
A model of this kind protects against both resistance and enthusiasm. It prevents leaders from rejecting AI without examining potential benefit, and it prevents them from adopting AI because modern language is persuasive. It asks the laboratory to show where the benefit will be realized and where the burden will be carried.
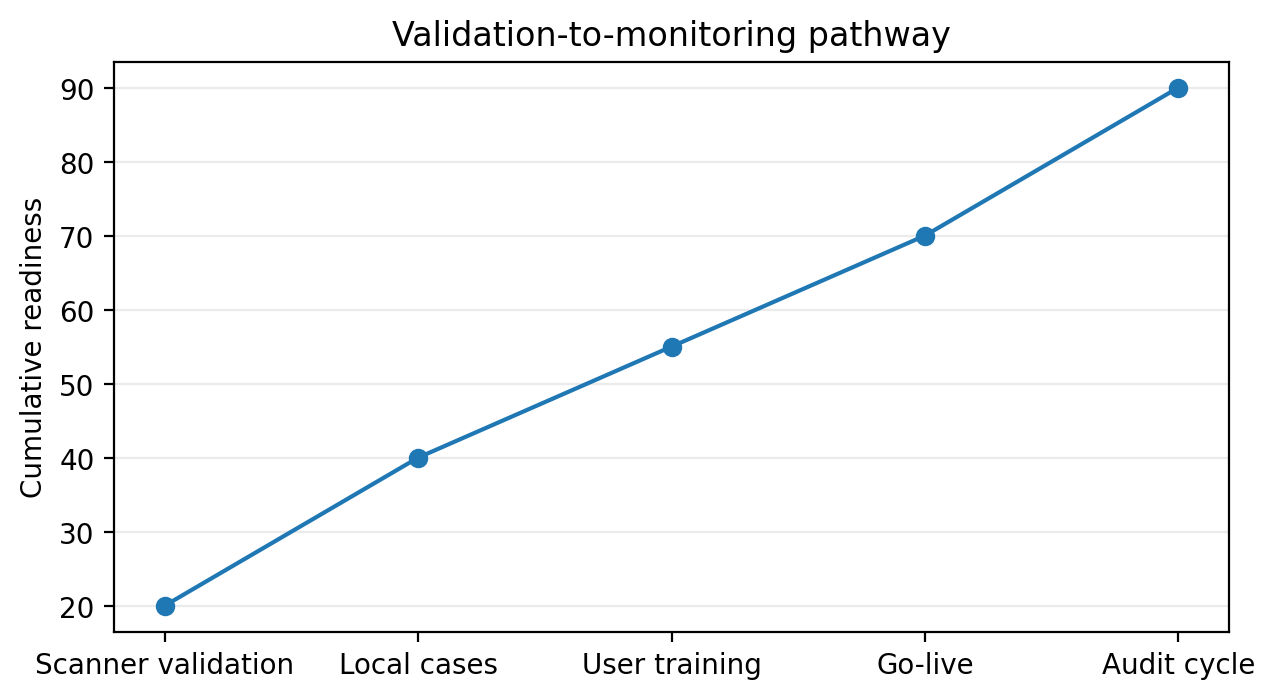
Figure 3. Author-developed visual prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved.
Table 2. Diagnostic-load balance model variables
| Variable | Meaning | Local evidence |
| V | Validated infrastructure | Scanner/display validation, image-quality logs. |
| A | Assistive review value | Alert usefulness, user review feedback. |
| E | Workflow efficiency | Turnaround time, click burden, case routing. |
| F | Workforce flexibility | Remote review, consultation, staff coverage. |
| R | Error risk | Discrepancies, missed/false alerts, excluded cases. |
| B | Implementation burden | Training, support, cybersecurity, monitoring workload. |
Note. Variables are author-developed planning variables, not private clinical data.
Chapter 7: Governance, Accountability, and Monitoring
7.1 Governance structure
AI-assisted digital pathology needs a defined governance structure before routine clinical use. A pathology AI committee or equivalent clinical governance forum can bring together pathologists, laboratory managers, informatics staff, cybersecurity leads, quality officers, procurement, data protection personnel, and patient safety representatives. The point is not to create a larger committee. The point is to place all relevant risks in one accountable forum.
Decision rights are explicit. Who approves go-live? Who authorizes a software update? Who reviews discrepancy events? Who can suspend use if image quality fails or alert behavior changes? Who communicates with clinicians if turnaround is affected? These decisions cannot be left to informal goodwill because diagnostic services operate under pressure.
Governance needs a record. Minutes, validation files, training logs, incident records, discrepancy reviews, and user feedback provide the history of the system. If an adverse event occurs, the laboratory shows not just that the device was authorized, but that the service was governed responsibly.
7.2 Cybersecurity and data control
Digital slides are patient data. They contain diagnostic material, identifiers, and sometimes links to clinical histories. AI-assisted pathology therefore raises cybersecurity and privacy duties that are not optional add-ons. Access control, encryption, logging, backup, vendor connectivity, and incident response all belong to the clinical safety case.
Cybersecurity failure in a pathology service can be more than a privacy breach. It can interrupt diagnosis, delay reporting, corrupt confidence in data, or compromise availability of prior slides. Health-service leaders can treat digital pathology infrastructure as critical clinical infrastructure. A laboratory that cannot access images or verify integrity cannot deliver diagnosis safely.
Vendor relationships require particular care. Contracts can address data use, update control, service availability, support response, security obligations, audit rights, and exit arrangements. Procurement cannot be separated from clinical governance. The terms under which data, software, and support are managed will affect diagnostic service quality.
7.3 Monitoring after implementation
Post-implementation monitoring is the difference between launch and learning. The laboratory can know whether the tool changes turnaround time, review behavior, case routing, discrepancy patterns, alert burden, user confidence, and consultation demand. Without monitoring, adoption becomes an act of faith.
Monitoring preserves professional judgment. A pathologist’s disagreement with software is not automatically an error, and a software alert is not automatically correct. The audit process can examine cases carefully, looking at the tissue, context, report, and user behavior. A crude scorecard could punish appropriate clinical independence.
The monitoring cycle can lead to action. If a recurring artifact creates false alerts, the scanning or preparation process needs review. If users report workflow friction, the interface or local routine needs change. If discrepancy review identifies a pattern, training or scope may need adjustment. AI governance earns trust when it changes practice in response to evidence.
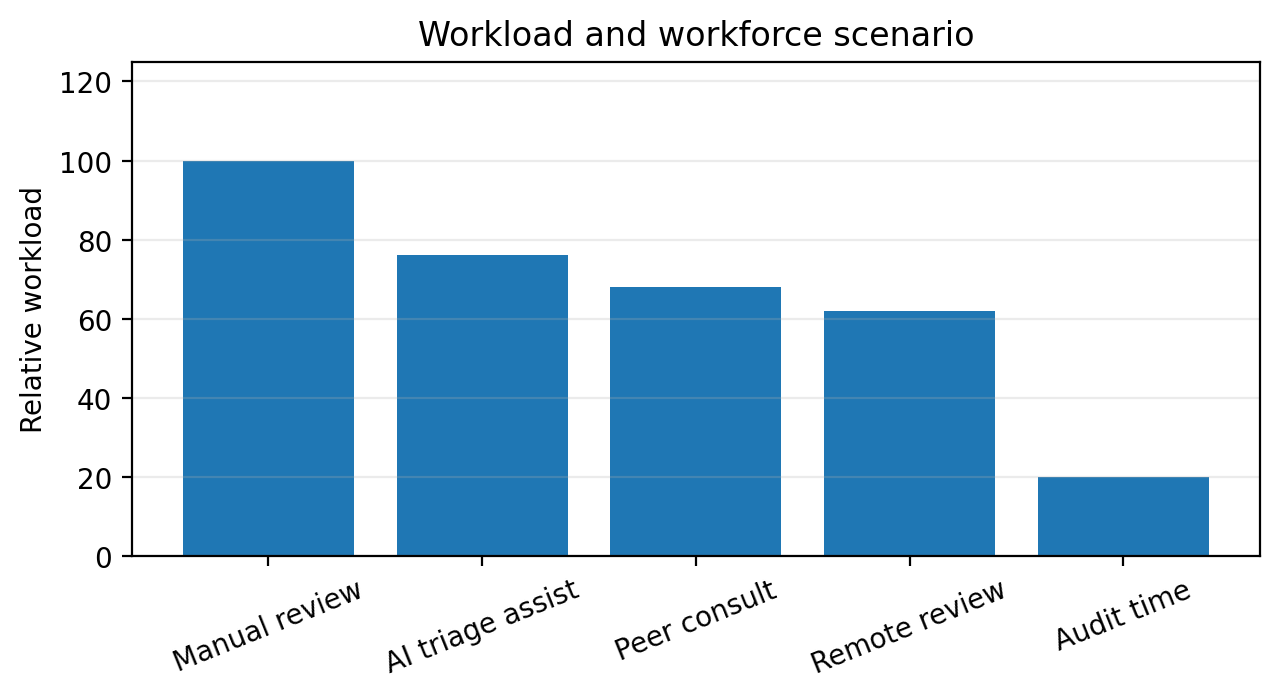
Figure 4. Author-developed visual prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved.
Chapter 8: Implementation Priorities
8.1 Readiness assessment
Implementation begins with readiness. A site can know whether whole-slide imaging is already validated for relevant diagnostic purposes, whether scanner capacity can handle the expected load, whether storage and network performance are reliable, whether displays meet diagnostic needs, and whether pathologists have time to participate in validation. These are not IT questions alone. They are diagnostic service questions.
Readiness assessment is documented in plain language. Boards and senior leaders require an understanding of the clinical path, not just the procurement logic. The assessment states what the tool will be used for, what it will not be used for, what evidence supports the use, what local validation showed, what burdens remain, and what conditions would trigger review.
The site can decide the launch route. A phased rollout may begin with a limited group of trained users and a defined case type. Early months can then be treated as a supervised period with active feedback. Broad rollout without early learning may look efficient, but it exposes the service to wider variation before the local system understands its own weak points.
8.2 Patient and clinician communication
Patients do not need a technical tutorial on AI, but they deserve truthful communication when diagnostic services change in ways that affect care. Clinical teams need language that explains assistive review without implying that diagnosis is being handed to software. The message is simple: digital tools may support review, while the pathologist remains responsible for diagnosis.
Referring clinicians need clarity. They requires knowledge of whether AI assistance affects report timing, case selection, consultation, or escalation. If a service is in phased rollout, clinicians require knowledge of what that means. Ambiguity can create anxiety, especially in cancer pathways where patients and treating teams are waiting for decisive reports.
Communication helps protect trust after problems. If a technical fault delays reporting or a software update requires temporary suspension, the service needs a plan for informing affected clinical teams. Silence is rarely neutral in cancer services. It can turn a manageable delay into loss of confidence.
8.3 Procurement and cost realism
Procurement can count the whole system. The cost of AI-assisted digital pathology includes software, scanner capacity, storage, network infrastructure, cybersecurity, validation time, staff training, quality review, support, and ongoing monitoring. A narrow licensing cost can make the investment appear simpler than it is.
Cost realism is not hostility to innovation. It protects innovation from backlash. When leaders approve a project on unrealistic assumptions, implementation teams are left to absorb the hidden work. The result may be delayed launch, frustrated pathologists, insecure workarounds, and weakened credibility. A better business case names the work honestly before approval.
The cost case can include potential value: reduced review delay, improved consultation, more flexible staffing, earlier identification of suspicious foci, and better audit. These benefits need local evidence. A service cannot manage what it refuses to measure.
Chapter 9: Extended Professional Analysis
9.1 Equity and access
AI-assisted digital pathology can widen access to expertise, but it can deepen inequity if only well-funded centers can implement it safely. A pathology service in a large academic hospital may have mature scanning infrastructure, informatics teams, and digital governance. A smaller service may face older systems, fewer pathologists, weaker network support, or limited capital. If adoption becomes a symbol of prestige rather than a pathway to safer diagnosis, the gap between institutions may grow.
Equity appears within the evidence base. Algorithms are trained and tested on particular slide preparations, scanners, staining patterns, populations, and case distributions. Local validation asks whether the local tissue, workflow, and patient population are adequately represented. A tool that works well in one setting may not perform the same way elsewhere.
Access to diagnostic quality matters because cancer care is time-sensitive and geographically uneven. Digital pathology can support expert review across distance, but only if infrastructure reaches beyond the better-resourced center. Policy leaders can view digital pathology as part of cancer-service capacity, not just as a laboratory modernization project.
9.2 Ethics of professional dependence
The ethical question is not whether pathologists may use tools. Medicine has always used tools. The question is whether the tool changes dependence in a way that weakens judgment. If a clinician gradually stops looking as carefully because software has become familiar, safety declines. If software highlights a region and the clinician checks more carefully, safety may improve.
Professional dependence is shaped by culture. A laboratory can cultivate careful use by encouraging challenge, documenting disagreement, reviewing missed or false alerts, and refusing to frame AI as superior to the pathologist. A vendor can support ethical use by being clear about intended use and limitations. A governance board can support ethical use by refusing exaggerated claims.
Ethical implementation requires accountability to patients. A patient harmed by diagnostic delay or error cannot face an institution that says the software did it or the pathologist did it without explaining the pathway. Responsibility in AI-assisted diagnosis is legible. The human system that adopted the tool remains answerable for the conditions of use.
9.3 Research needs
Future research can move beyond adoption narratives. Laboratories need evidence about turnaround time, discrepancy patterns, false-alert burden, user confidence, training quality, cost, equity, and patient-level outcomes after implementation. Evidence from controlled studies is important, but service evidence is different. It shows whether the tool survives real laboratory life.
Multi-site studies would be especially valuable because digital pathology systems vary. Scanner models, staining practices, case mix, staffing, local validation, and reporting habits differ across sites. A study that works in one institution may not answer questions for another. General claims are supported by diverse settings.
Research requires workforce experience. Pathologists and laboratory staff can explain whether the tool reduces cognitive load, adds friction, supports consultation, or creates new administrative tasks. Without that evidence, leaders may mistake technical performance for service success.
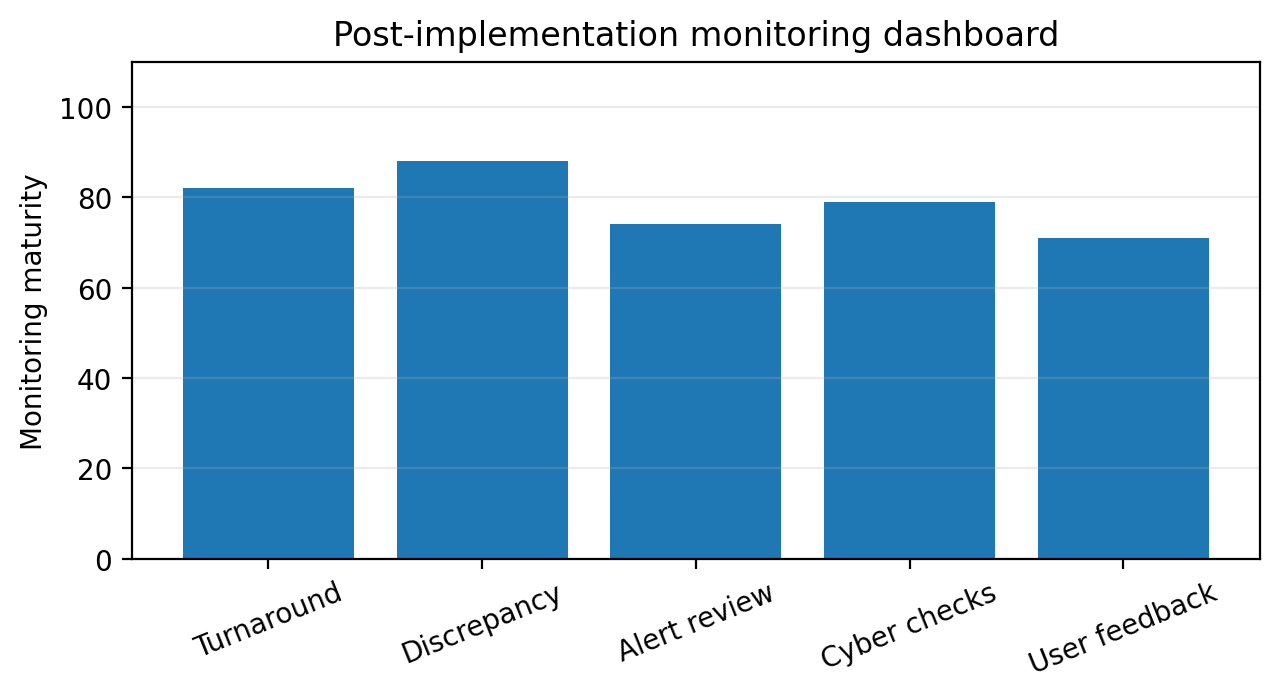
Figure 5. Author-developed visual prepared for NYCAR publication use. Copyright © June 2026 Ogochukwu I. Okoye. All rights reserved.
Chapter 10: Recommendations and Final Position
10.1 Recommendations
Laboratories considering Paige Prostate or similar tools can begin with intended use. The software is used only for the case types and purposes supported by the regulatory and local validation record. Intended use belongs in training, protocols, audit, and case selection. It cannot remain a sentence in a procurement file.
Whole-slide imaging validation is complete before AI support becomes routine. Scanner performance, image quality, display conditions, viewer usability, and case equivalence need documentation. The laboratory can keep a validation file that a clinical governance board can understand.
Pathologist authority needs explicit protection. Reports remain signed by responsible pathologists. Disagreement with software is possible, recordable, and reviewable. No productivity target can imply that algorithmic highlighting reduces the duty of diagnostic review.
Post-implementation monitoring can begin at launch. Turnaround time, discrepancy review, alert burden, user feedback, technical downtime, cybersecurity events, and excluded cases is reviewed on a defined schedule. Early problems can produce local changes, not quiet tolerance.
Cybersecurity and data control is governed as clinical safety issues. Slide images, patient identifiers, access logs, vendor connectivity, backups, and incident response need clinical oversight as technical management. The laboratory cannot diagnose safely if the digital record is unavailable, insecure, or untrusted.
10.2 Final position
The final position of this publication is cautious in form and constructive in purpose. Paige Prostate shows that AI-assisted pathology has moved from speculation into regulated clinical support. That is important. It does not mean that laboratories can buy diagnostic safety in a software package.
The value of AI-assisted pathology appears when the laboratory already has the discipline to use it: validated digital infrastructure, trained pathologists, documented workflow, clear governance, protected data, and continuous monitoring. Without those conditions, the technology may still look advanced, but the patient’s diagnostic pathway may become harder to trust.
Digital pathology is therefore a test of health-service maturity. A mature service welcomes tools that support diagnostic attention while refusing to surrender judgment. It measures improvement rather than assuming it. It protects the workforce rather than treating staff as an obstacle to automation. It explains responsibility clearly. That is the standard a clinical AI program can meet.
Chapter 11: Applied Laboratory Assurance Protocol
11.1 Evidence register for local use
A laboratory that adopts assistive AI needs an evidence register that does more than store vendor paperwork. The register can show what the laboratory knows about the system it is using, how that knowledge was produced, and which decisions follow from it. A useful register begins with intended use, scanner and viewer validation, image-quality criteria, user training records, local case-set review, discrepancy review rules, cybersecurity approvals, and update-control procedures.
The evidence register is written for several audiences. Pathologists require knowledge of how the system behaves during review. Laboratory managers require knowledge of staffing, maintenance, and turnaround effects. Information-governance staff require knowledge of how patient images move and where they are stored. Senior leaders require knowledge of what risk the organization has accepted. The register is therefore a translation tool as much as a compliance record.
A weak register produces predictable confusion. When software is updated, nobody knows whether local validation is repeated. When a scanner is replaced, nobody knows whether images remain equivalent. When a pathologist questions an alert, nobody knows whether the event belongs in quality review. When cybersecurity arrangements change, nobody knows whether clinical staff need new instructions. The register reduces those gaps because it keeps the service history in one place.
The register can contain exceptions, not just approvals. If a case type is excluded, the reason belongs in the record. If an alert category is considered unreliable, that fact belongs in the record. If the launch is limited to a defined user group, the boundary belongs in the record. An evidence register that records only success tells the least useful part of the story.
11.2 Local validation set design
Local validation needs a case set that reflects the work the laboratory plans to do. Prostate biopsy material requires a range of benign cores, small suspicious foci, definite carcinoma, artifacts, inflammation, common mimics, and image-quality variation. The point is not to create a perfect experimental study. The point is to prevent the laboratory from learning too late that local material differs from assumptions made during procurement.
Case-set design is reviewed by pathologists who understand the local diagnostic workload. Informatics teams can support file handling and image preparation, but they cannot decide alone whether the cases are diagnostically adequate for validation. The professional eye of the pathologist remains central because the danger lies in clinical nuance, not just pixel quality.
Validation results is discussed in terms of decisions. If the tool performs acceptably only when images are of a certain quality, the service needs an image-quality gate. If users disagree about how to respond to alerts, the training material needs revision. If review time increases during early use, the rollout plan may need a slower schedule. Validation is useful only when it changes how the service is managed.
A good validation protocol protects against retrospective storytelling. Without predefined criteria, teams may explain away weak results because the project already has momentum. Criteria is agreed in advance: acceptable discrepancy, user confidence, turnaround effect, technical failure, and escalation triggers. Predefinition makes local judgment fairer.
11.3 Update control and version accountability
Software systems change. That fact is often treated as ordinary IT maintenance, but in clinical AI it may affect diagnostic behavior. A minor interface adjustment can change how an alert is noticed. A model update can change sensitivity, specificity, or the pattern of highlighted regions. A viewer update can change performance or user navigation. A laboratory that does not govern versions cannot confidently explain what system produced a given clinical condition.
Version accountability requires a policy. The policy states how software updates are announced, who reviews them, what level of revalidation is required, how users are informed, and how the change is recorded. Some updates may require only technical confirmation. Others may require renewed clinical testing. The difference cannot be left to the vendor alone.
Update control matters for retrospective review. If a discrepancy is found six months after a report, the laboratory may require knowledge of which software version, scanner, viewer, and workflow were in use at the time. A system without version history makes accountability harder. This is not administrative excess. It is the record needed to understand clinical events.
The safest update culture is neither rigid nor careless. It allows improvement while protecting clinical evidence. New versions may bring better performance, but each change needs an accountable route into practice.
Chapter 12: Patient Safety, Equity, and Public Trust
12.1 The patient behind the slide
Digital pathology writing can become abstract because slides, algorithms, scanners, and dashboards dominate the language. Patient safety requires the opposite discipline. Behind every prostate biopsy is a person waiting for a result that may lead to surveillance, surgery, radiotherapy, systemic treatment, or relief. Turnaround time, accuracy, clarity, and continuity matter because a report enters a life, not just a database.
The patient rarely sees the laboratory, yet the laboratory shapes the patient’s options. A delayed report can postpone the next appointment. An unclear report can complicate clinical explanation. A missed focus can delay cancer recognition. An overcalled finding can lead to anxiety and unnecessary intervention. These consequences give digital pathology its ethical weight.
AI assistance can therefore be judged by what it does to the patient pathway. Does it help reports become safer and timelier? Does it support clinicians with clearer information? Does it reduce bottlenecks in consultation? Does it introduce unexplained variation? Does it widen access for patients in sites with limited subspecialty expertise? These questions keep the system honest.
12.2 Equity in digital implementation
Equity concerns arise in several places. Wealthier health systems may adopt digital pathology earlier, while lower-resource services remain dependent on older infrastructure. Urban centers may gain subspecialty digital networks while smaller hospitals struggle with scanner procurement or network reliability. If digital pathology becomes a premium capability rather than a shared diagnostic asset, patients may experience uneven access to advanced review.
Equity concerns data. AI systems reflect the material used to develop and test them. Tissue preparation, scanner types, staining practices, and case populations vary. Local validation provides one safeguard, but it cannot answer every population question. Laboratories can watch for patterns in which the system behaves differently across preparation methods, case sources, or patient groups.
An equity-minded implementation plan includes access, geography, and service distribution. It asks whether remote review can help under-served areas, whether network costs will exclude smaller sites, whether staff in all settings receive adequate training, and whether patient pathways are improved where diagnostic delay is greatest. Digital pathology can support fairness only when fairness is part of the design.
12.3 Public trust and explanation
Public trust in medical AI is fragile because patients may hear the word artificial intelligence and imagine replacement, surveillance, or experimentation. A health service that uses AI-assisted review needs language that is factual and calm. The patient can understand that the pathologist remains responsible, that the tool is used within an approved and validated pathway, and that the purpose is to support careful review.
Overpromising damages trust. Claiming that AI removes error or solves workforce pressure will eventually collide with real clinical complexity. Underexplaining damages trust. If patients discover later that AI was used and the service never explained how responsibility was protected, suspicion may follow. The correct public voice is direct: the tool may support review; the diagnosis remains a professional act; the laboratory monitors the service.
Explanation is needed inside the organization. Clinicians who receive reports requires knowledge of the service pathway well enough to answer patient questions. Laboratory staff requires knowledge of what is being implemented and why. Governance teams can understand the evidence. Trust is built when explanation travels with the technology.
Appendix A: NYCAR Implementation Checklist for AI-Assisted Digital Pathology
A.1 Governance checklist
The implementation checklist begins with a question that is often skipped because it sounds too simple: what exactly is the system intended to do in this laboratory? The answer can name the specimen type, user group, scanner pathway, review sequence, reporting effect, exclusion criteria, and decision owner. If the answer cannot be written clearly, the service is not ready for launch.
The governance checklist requires: intended use statement; local validation approval; named clinical lead; named laboratory operations lead; information-governance review; cybersecurity approval; vendor-support route; version-control rule; incident-reporting route; discrepancy-review schedule; user training log; patient and clinician communication plan; and suspension criteria. Each item needs an owner and a date.
The checklist is not designed to slow useful technology. It prevents ambiguity from becoming clinical risk. A laboratory under pressure may want to move quickly, yet speed without accountable preparation creates future delay. The checklist gives leaders a way to move with discipline.
A.2 Monitoring checklist
Monitoring begins with the everyday questions of the service. Are reports being completed on time? Are pathologists comfortable using the tool? Are alerts clinically useful? Are there repeated false signals? Are cases being excluded for image-quality reasons? Are scanner or viewer problems delaying review? Are cybersecurity or access problems affecting availability?
The monitoring file can contain numerical measures and narrative review. Numbers may show that turnaround time improved, but users may still report frustrating alert placement. Numbers may show few discrepancies, but a small number of serious events may require immediate action. Narrative review prevents metrics from becoming a substitute for professional judgment.
An annual review asks whether the tool remains fit for purpose. The answer may be yes, but it is earned. The service may need updated training, revalidation after software changes, review of excluded cases, or revised governance if the case mix has changed. Continuing use is a decision, not an assumption.
A.3 Evidence table
A final evidence table is maintained by the laboratory. It lists each source of evidence, the date reviewed, the decision made, and the next review point. FDA material, CAP guidance, local validation, user feedback, discrepancy review, technical incident records, cybersecurity review, and patient-pathway metrics belong in the same governance file because they describe one clinical service.
The value of this table appears when something goes wrong. Leaders can see what was known, what was decided, and where the service may have failed. That visibility supports learning. It protects staff from vague blame because the pathway becomes easier to reconstruct.
AI-assisted digital pathology will continue to develop. New tools will extend beyond prostate biopsy review into other tissues, tasks, and reporting practices. The checklist in this appendix gives laboratories a practical way to evaluate each new claim: define the use, validate locally, protect professional authority, monitor after launch, and keep the patient’s diagnostic pathway at the center.
Chapter 13: Case Scenarios in Diagnostic Governance
13.1 Small focus in a high-volume session
A useful way to test the governance framework is to imagine an ordinary high-volume reporting session. The pathologist is reviewing many prostate biopsy cores. Most are benign. The danger is not dramatic incompetence; it is fatigue, repetition, time pressure, and a small suspicious focus that does not announce itself. In that setting, assistive software may have value because it can direct attention to a region that deserves careful inspection.
The managerial point is not that the software becomes the diagnostician. The point is that the service has created a The next point layer of attention inside a repetitive task. If the alert is well integrated, the pathologist can examine the region, agree or disagree, and continue with professional control. If the alert is poorly integrated, it may distract, slow review, or create doubt without adding useful information.
A governance review of this scenario would examine whether the pathologist saw the alert, whether the alert was clinically appropriate, whether review time changed, and whether the final report reflected independent interpretation. This case raises training questions. Pathologists require knowledge of how to respond to low-confidence, high-confidence, and apparently mistaken signals without turning the software into either an authority or an annoyance.
The scenario is ordinary, which is why it matters. Patient safety is often protected not by rare heroic interventions but by better design of repeated work. If AI assistance reduces the chance that a small focus is missed during routine review, the effect may be clinically meaningful. That benefit still depends on validation, usability, and monitoring.
13.2 Image-quality failure
Another scenario begins with a flawed scan. The tissue may be folded, focus may be weak, staining may be uneven, or an image tile may fail. A human pathologist may notice the problem because the image feels wrong during review. An algorithm may behave unpredictably because the image no longer matches the expected input. The service needs a rule for this situation before it occurs.
Image-quality failure is not a minor technical event. It can alter diagnostic confidence. The laboratory needs a process for identifying poor scans, rescanning, excluding cases from AI support, and documenting the decision. The scanner operator, pathologist, and quality lead all have roles. A system that sends poor images into assisted review without a gate is placing software into a setting it was not designed to manage.
Monitoring image-quality failures can reveal deeper service issues. A recurring focus problem may point to scanner maintenance. A staining variation may point to laboratory preparation. A pattern in particular specimen types may require additional validation. The AI tool becomes part of a wider quality conversation because its behavior depends on the images it receives.
The safest service culture treats technical faults as clinical information. Staff are encouraged to report poor images, pathologists are supported when they request rescanning, and leadership sees the cost of rescanning as part of diagnostic protection rather than wasted time.
13.3 Remote consultation under pressure
A The final point scenario involves remote consultation. A smaller hospital scans a prostate biopsy case and seeks subspecialty input from a pathologist at another site. Digital pathology makes that consultation easier because the slide can move without moving glass. AI assistance may help identify regions for discussion. The patient may benefit from faster access to expertise.
Remote consultation still requires a controlled pathway. The receiving pathologist needs adequate display conditions, secure access, case context, clinical history, and a reporting route. The originating laboratory can know how the consultation will be documented and how responsibility is shared. If software alerts are used, the consultative record can make clear whether they informed discussion or whether the consultant conducted a separate review.
This scenario shows why digital pathology can be a workforce strategy. Scarce expertise can be distributed across geography. Services can collaborate without courier delays. Yet the governance becomes more complicated because multiple organizations, systems, and professionals may be involved. Contracts, data-sharing rules, indemnity, response times, and quality review all need attention.
The practical lesson is that remote review is not less formal than on-site review. It may require more explicit governance because the familiar cues of the local laboratory are absent. A digital consultation pathway that is secure, documented, and clinically clear can improve access. An informal pathway can create new uncertainty.
Chapter 14: Management Metrics and Board Assurance
14.1 Board-level indicators
A board or senior clinical governance committee does not can see every software alert. It does need a small set of indicators that reveal whether the service remains safe and useful. Suitable board-level indicators include validated case scope, turnaround time, excluded cases, image-quality failures, discrepancy-review outcomes, user feedback, cybersecurity incidents, software version status, and training completion.
The point of board assurance is not to pull diagnostic judgment into executive meetings. It is to ensure that leaders who approve investment and risk understand whether the system they authorized is behaving as expected. AI-assisted pathology may be technically complex, but its assurance questions can be made legible: is it being used for the approved purpose, is it reliable in local use, are staff prepared, are exceptions managed, and is patient care affected?
A board report can separate facts from interpretation. Facts include numbers: number of cases reviewed, excluded scans, average turnaround time, discrepancy events, downtime, training completion. Interpretation explains what those numbers mean. A rising exclusion rate may indicate poor image quality, more cautious users, or better detection of unsuitable cases. Governance requires explanation, not just counting.
The board can see unresolved risks. If an update is pending, if storage capacity is under pressure, if a user group has not completed training, or if turnaround gains have not appeared, those points belong in the report. Mature governance does not hide uncertainty until after harm.
14.2 Laboratory-level metrics
Laboratory leaders need a more detailed view than the board. They require knowledge of where work slows, where staff struggle, which cases are excluded, how often rescanning occurs, whether alerts are useful, and how frequently users disagree with the system. These metrics belong close to the people doing the work because they can change practice quickly.
Useful laboratory measures include scan-to-view time, view-to-report time, rescan rate, AI-alert review time, report amendment frequency, consultation rate, and technical-support response time. Some measures will be affected by case complexity, so leaders can interpret trends with pathologist input. A higher consultation rate may indicate uncertainty, but it may indicate better use of expertise.
Metrics cannot be weaponized against pathologists. If users fear that disagreement or slower review will be judged as failure, they may stop reporting useful concerns. Early implementation needs a learning culture. The goal is to understand how the service behaves, not to produce a perfect dashboard.
A laboratory metric is valuable when it leads to change. If scan-to-view time is slow, network or storage performance may need work. If rescan rates rise, slide preparation or scanner maintenance may be at issue. If alert burden is high, training or case-scope refinement may be needed. The metric is the beginning of action, not its substitute.
14.3 Patient-pathway metrics
Patient-pathway metrics connect the laboratory to the wider cancer service. A pathology report enters a chain that includes the urologist, multidisciplinary team, treatment planning, and patient communication. If the AI-assisted pathway improves internal laboratory measures but has no effect on patient-facing timelines, the service can understand why.
Patient-pathway metrics might include biopsy-to-report time, report-to-clinician review time, report-to-MDT time, and report-to-treatment decision time. The laboratory does not control every part of that chain, but it influences it. A diagnostic service that sees only its own turnaround may miss the point at which diagnostic delay reappears elsewhere.
These metrics help justify investment. Senior leaders are more likely to support digital pathology when the service can show effects beyond internal efficiency. A faster and safer report can contribute to cancer pathway performance, clinician confidence, and patient reassurance. The benefit becomes visible when it is linked to the path the patient actually travels.
Patient-pathway measures need careful interpretation because improvement may be blocked by downstream constraints. If reports are faster but treatment appointments remain delayed, the pathology service has still improved its part of the system. The lesson is that diagnostic innovation and wider cancer capacity are governed together.
Chapter 15: Research Limits and Future Agenda
15.1 Limits of public evidence
This publication relies on public regulatory and professional evidence. That is appropriate for a master’s research publication, but it creates limits. Public evidence can describe authorization, intended use, guidelines, and published concerns. It cannot show every private laboratory decision, every user experience, every local discrepancy, or every vendor support event. A reader can therefore treat the framework as a disciplined planning model rather than a completed evaluation of all Paige Prostate deployments.
The limits are not a weakness when they are named. Many institutional publications lose credibility because they pretend to have more data than they actually have. This study does not report private coefficients, hidden patient outcomes, or confidential performance logs. It identifies the data that responsible organizations would can collect.
Those data include local validation results, case exclusions, alert patterns, user disagreement, turnaround time, discrepancy review, technical downtime, training completion, update history, and patient-pathway effects. A hospital or laboratory adopting AI-assisted pathology could use those data to produce a much more reliable empirical study after implementation.
The research position is therefore modest and useful. Public evidence supports the case for careful adoption. Local evidence decides whether adoption has improved the service.
15.2 Future research questions
Future research can examine AI-assisted pathology in real laboratory workflows across multiple sites. A useful study would compare sites with different scanners, case volumes, staffing patterns, digital maturity, and governance models. It would ask whether AI assistance changes diagnostic turnaround, pathologist workload, discrepancy rates, consultation patterns, and user confidence. It would not stop at accuracy.
Research can examine patient communication. Patients may respond differently to the use of AI in diagnosis depending on how it is explained, whether responsibility is clear, and whether the service has public trust. A patient-centered study could examine what language supports understanding without creating fear or false certainty.
Workforce studies are needed because AI adoption can be felt differently by pathologists, laboratory scientists, informatics teams, and managers. The same tool may reduce one kind of work while increasing another. A serious workforce study would examine transition burden, training time, troubleshooting, remote review, peer consultation, and job satisfaction.
Equity research can examine whether digital pathology and AI assistance reduce geographic variation in diagnostic access or widen it. If high-resource centers gain better tools while lower-resource centers fall behind, the technology may improve some services while leaving structural inequity intact. Equity is measured, not assumed.
15.3 Closing research statement
Digital pathology and AI-assisted diagnosis will keep moving. The question for health systems is not whether the field can be stopped. It cannot. The question is whether adoption will be governed with enough clinical discipline to protect patients and enough workforce realism to protect the professionals who carry diagnostic responsibility.
Paige Prostate is a valuable case because it keeps the discussion concrete. It shows a defined device, a defined intended use, a defined diagnostic field, and a defined human role. That specificity allows better thinking. Instead of asking whether AI is good or bad for medicine, the study asks how one assistive system can be governed in one sensitive diagnostic pathway.
The answer is neither rejection nor celebration. The answer is stewardship. Validate the digital pathway. Protect pathologist authority. Monitor performance. Count the implementation burden. Respect patient trust. Use AI where it supports diagnostic attention, and refuse to let the language of innovation outrun the conditions of safe clinical use.
Appendix B: Diagnostic Incident Review Scenarios
B.1 Discrepant case after sign-out
A discrepant case after sign-out is the moment when governance becomes visible. Suppose a later review identifies a suspicious focus that was not included in the original report. The laboratory’s The opening point obligation is clinical: determine whether the patient’s care needs correction and whether the treating team requires immediate information. The next obligation is analytic: reconstruct the pathway without rushing to a convenient explanation.
The review file can identify the original slide, scanner, software version, user, case context, image quality, alert behavior, report timing, and any peer consultation. If the AI tool highlighted the region and the pathologist did not agree, the review asks how the disagreement was handled. If the AI tool did not highlight the region, the review asks whether this case falls outside expected behavior or whether a pattern is emerging. If the image was poor, the review asks why it passed the quality gate.
This process protects fairness to staff because it avoids shallow blame. A missed focus can arise from tissue quality, scanning, workflow pressure, communication, or interpretation. The review can identify the system conditions that made the event possible. It can then decide whether training, case selection, scanning practice, peer review, or monitoring thresholds need change.
The result of a discrepant-case review is recorded in a form that can be learned from later. If the same type of problem appears again, the laboratory cannot can rediscover the earlier lesson. A diagnostic incident has value only if it changes the probability of repetition.
B.2 Vendor-supported investigation
Some events will require vendor involvement. A laboratory may observe unusual alert behavior, performance slowing, display problems, or suspected software malfunction. Vendor support can be essential, but the laboratory remains responsible for clinical governance. A vendor investigation cannot replace internal assessment of patient impact.
The service needs rules for vendor-supported review. What data may be shared? How are patient identifiers protected? Who authorizes transfer? What timeline applies? How is the vendor’s response reviewed by clinical staff? How is the event recorded? These details can exist before an incident, because urgent situations are poor times to design data-governance rules.
A vendor may provide technical explanations, log review, patch information, or guidance. Clinical leaders then decide what those explanations mean for diagnostic practice. If the issue affects a past case, clinical review is needed. If it affects future cases, scope or use may need temporary restriction. If it affects trust in a software version, update control becomes central.
Vendor relationships are most reliable when they are honest and bounded. The vendor knows the product. The laboratory knows the patient pathway. Good governance uses both forms of knowledge without confusing their responsibilities.
B.3 Temporary suspension of AI support
A mature service knows how to pause. Temporary suspension is not failure when evidence requires caution. It is one of the signs that governance has authority. If image-quality failure rises, if software behavior changes after update, if cybersecurity access is in question, or if users report serious concern, the laboratory may can suspend assisted use while continuing diagnostic work through validated conventional or digital review pathways.
Suspension criteria is written before launch. The criteria may include unresolved serious discrepancy, unknown software behavior, inability to access images securely, major scanner fault, failed version-control review, or inadequate user training after staff change. The criteria give staff confidence that safety will not be negotiated under pressure.
A suspension plan can name the alternative workflow. Cases may be reviewed without AI assistance, sent for peer review, routed to another validated scanner, or held for rescanning depending on urgency and clinical need. The patient pathway remains the priority. The suspension cannot become an excuse for unmanaged delay.
Restart needs criteria. The service cannot resume because everyone is tired of the pause. It can resume when the relevant issue has been investigated, the corrective action is recorded, users have been informed, and governance has accepted the residual risk.
B.4 Training after a learning event
A learning event becomes useful only when staff understand it. If a discrepancy review, image-quality problem, or workflow incident reveals a pattern, training can convert that finding into practice. Training after an event is different from launch training. It is grounded in a real weakness found in local use.
The training is specific. It may show a de-identified example of poor focus, explain when to request rescanning, clarify how to document disagreement with an alert, revise the escalation pathway, or remind users of intended-use boundaries. General reminders rarely change practice. Specific lessons do.
Training can respect professional dignity. The aim is not to shame the person closest to the incident. It is to help the service learn. A staff member who reports a problem cannot become the problem. If reporting is punished, the service will become quieter and less safe.
The final test of training is whether behavior changes. The laboratory can examine subsequent cases, user feedback, and event rates to see whether the lesson entered routine work. Education is not complete when slides are presented. It is complete when the safer habit appears in practice.
Appendix C: Variable Definitions for Local Evaluation
C.1 Diagnostic and workflow variables
Local evaluation requires variable definitions that staff can use consistently. “Turnaround time” can specify start and end points: receipt to scan, scan to pathologist view, view to report, or biopsy to clinician review. “Image-quality failure” can specify whether the problem concerns focus, tissue coverage, color, artifact, tile failure, file corruption, or display. “AI alert review” can specify whether the pathologist saw, examined, accepted, rejected, or ignored the alert.
“Discrepancy” cannot be a vague label. It can indicate whether the discrepancy concerns diagnostic category, grade, suspicious focus, report clarity, technical exclusion, or case routing. Different discrepancy types require different responses. A category-level diagnostic disagreement is not the same as a minor formatting issue in a report.
“Workflow friction” is captured through user reporting and observation. It may include slow image loading, excessive clicks, confusing alert display, difficulty returning to a region, mismatch between viewer and reporting system, or unclear case status. These points matter because they shape whether the tool can be used carefully during real diagnostic sessions.
Each variable requires a data owner. Without ownership, data collection collapses into aspiration. Scanner staff may own rescan rates; pathologists may own discrepancy classification; informatics staff may own downtime; governance may own review actions. Clear ownership turns evaluation from an idea into a routine.
C.2 Workforce and equity variables
Workforce variables requires user group, training completion, supervised-use period, review volume, overtime pressure, consultation demand, remote review use, and reported confidence. The aim is not surveillance of individuals. The aim is to understand whether the system helps or burdens the workforce.
Equity variables may include site type, referral source, geographic location, case-routing pattern, and access to subspecialty review. The laboratory can examine whether the digital pathway improves access beyond the central site or concentrates benefit where resources already exist. If AI-assisted digital pathology is treated as an equity tool, equity is measured.
Patient-pathway variables include biopsy-to-report time, report-to-clinician review, and report-to-treatment decision. These measures remind the service that diagnostic work belongs to a wider cancer journey. A laboratory metric that never reaches the patient pathway may be too narrow.
Evaluation remains proportionate. A small laboratory does not need an industrial analytics platform to begin. It can start with a clear register, a small dashboard, routine case review, and quarterly governance discussion. The discipline matters more than the polish of the spreadsheet.
C.3 Closing implementation note
The variables in this appendix are not a demand for endless measurement. They identify the minimum evidence needed to know whether an AI-assisted pathology pathway is becoming safer, slower, more useful, more burdensome, or more equitable. Without such evidence, leaders are left with impressions and vendor claims.
Local evaluation is revised after experience. Some variables may prove unhelpful. Others may become essential. The service can adapt the evaluation plan as it learns, while preserving enough consistency to detect trends over time.
The broader lesson is simple: clinical AI requires institutional memory. Every validation, update, incident, disagreement, training session, and monitoring review adds to what the laboratory knows about safe use. A service that records and acts on that knowledge becomes better. A service that forgets it is likely to repeat the same mistakes under a new name.
Appendix D: Board Assurance Questions
D.1 Questions for executives
Executives approving AI-assisted digital pathology need a line of inquiry that is plain enough for governance and serious enough for clinical risk. The opening question is whether the service can explain its intended use without relying on vendor language. If leaders cannot state where the tool fits, who uses it, what it supports, and what it does not do, the project is still too vague.
The next question is whether local validation has been reviewed by people with diagnostic authority. A board cannot accept a slide deck that says validation is complete without seeing the evidence category: case numbers, user groups, discrepancy findings, scanner environment, exclusion criteria, and sign-off. The board does not can read every case. It needs assurance that someone qualified has done so and that the result changed the implementation plan where needed.
Executives ask what will happen if the system is unavailable. A diagnostic service cannot be dependent on a tool without a fallback. If scanning fails, if the viewer is unavailable, if vendor support is delayed, or if a cybersecurity event restricts access, the laboratory needs a continuity pathway. The continuity plan is part of the decision to adopt.
A final executive question concerns benefit evidence. What will convince the institution after twelve months that the tool improved care or service resilience? The answer is written before launch. It may include reduced turnaround for qualifying cases, improved access to consultation, fewer avoidable rescans, better workload distribution, or clearer discrepancy review. If no benefit evidence is defined, the system may continue because it exists rather than because it helps.
D.2 Questions for pathology leaders
Pathology leaders ask whether the tool protects the diagnostic culture of the department. A healthy diagnostic culture allows disagreement, peer review, careful uncertainty, and escalation. If AI is introduced in a way that makes pathologists feel judged by a machine or hurried by productivity claims, culture may deteriorate. The leadership task is to make the tool serve professional practice rather than make professional practice serve the tool.
They ask how trainees and less experienced staff will encounter the system. AI support can educate attention, but it can distort learning if users treat highlights as the map of the case. Training can teach morphology The opening point and software behavior The next point. The pathologist has a duty to know why a region matters, not just that the system has marked it.
Pathology leaders can examine the impact on peer consultation. Digital workflows may make consultation easier, but they may reduce informal discussion if everyone works separately. Leaders can preserve the human spaces where difficult cases are discussed. Diagnostic quality depends on professional community as software.
The department can decide how it will handle skepticism. Some pathologists may distrust AI; others may be too eager. Both positions need evidence. The department can give users a structured way to raise concerns, compare cases, and influence local protocols. Adoption without professional ownership is brittle.
D.3 Questions for regulators and policy readers
Regulators and policy readers can use this case to see the difference between authorizing a device and building a diagnostic service. Authorization examines a defined product through a defined regulatory process. Service readiness examines whether local conditions can support safe use. Both are needed, and neither substitutes for the other.
Policy can encourage transparency around intended use, validation, monitoring, and responsibility. It can resist both blanket suspicion of clinical AI and blanket confidence in authorized products. The public interest lies in careful adoption: tools that improve attention and access, systems that remain accountable, and evidence that can be reviewed after implementation.
Digital pathology policy can consider smaller and lower-resource settings. If policy assumes that all laboratories can adopt at the speed of leading centers, it may widen variation. Support for shared infrastructure, regional networks, training, and cybersecurity may be necessary if AI-assisted pathology is to serve equity rather than prestige.
The final policy question is whether health systems can learn collectively. Each laboratory can monitor locally, but isolated learning is slow. De-identified implementation lessons, validation challenges, and workflow findings could help other services avoid repeated errors. The field will mature faster if clinical governance knowledge travels with technical progress.
D.4 Final assurance judgment
The final assurance judgment is not a slogan that the system is ready. It is a record of conditions. A proper judgment states that the intended use is defined, the digital pathway is validated, the users are trained, the clinical lead accepts the workflow, cybersecurity has been reviewed, monitoring is scheduled, and a suspension route exists if the evidence changes.
That judgment is dated and revisited. A service can be ready in June and less ready after a software update, staffing change, scanner replacement, or shift in case mix. Readiness is therefore a living condition. This is especially true in AI-assisted diagnosis, where the service depends on a relationship between people, images, software, and governance routines.
The professional lesson of the Paige Prostate case is that safety lives in the relationship among these parts. The scanner cannot replace the pathologist. The pathologist cannot compensate for a poorly governed digital environment forever. The vendor cannot own the patient pathway. The board cannot approve and then stop listening. The service is safe only when each actor understands the boundary of responsibility and the evidence that keeps the boundary honest.
For NYCAR purposes, this is the publication’s governing claim: clinical AI becomes worthy of trust only when its usefulness is carried by an accountable institution. A laboratory that can define, validate, monitor, pause, learn, and explain its AI-assisted work is not simply adopting technology. It is practicing diagnostic stewardship.
References
College of American Pathologists. (2025). Artificial intelligence in pathology resources. https://www.cap.org/member-resources/councils-committees/informatics-committee/artificial-intelligence-pathology-resources
Evans, A. J., Brown, R. W., Bui, M. M., Chlipala, E. A., Lacchetti, C., Milner, D. A., Pantanowitz, L., Parwani, A. V., Reid, K., Riben, M. W., & Validating Whole Slide Imaging Systems for Diagnostic Purposes in Pathology Guideline Update Expert Panel. (2022). Validating whole slide imaging systems for diagnostic purposes in pathology: Guideline update. Archives of Pathology & Laboratory Medicine, 146(4), 440–450.
International Organization for Standardization. (2023). ISO/IEC 42001:2023: Information technology—Artificial intelligence—Management system. ISO.
McGenity, C., Clarke, E. L., Jennings, C., Matthews, G., Cartlidge, C., Freduah-Agyemang, H., Stocken, D. D., & Treanor, D. (2024). Artificial intelligence in digital pathology: A systematic review and meta-analysis of diagnostic test accuracy. npj Digital Medicine, 7, Article 114. https://doi.org/10.1038/s41746-024-01106-8
National Institute of Standards and Technology. (2023). Artificial intelligence risk management framework (AI RMF 1.0). U.S. Department of Commerce. https://doi.org/10.6028/NIST.AI.100-1
Pantanowitz, L., Sinard, J. H., Henricks, W. H., Fatheree, L. A., Carter, A. B., Contis, L., Beckwith, B. A., Evans, A. J., Lal, A., & Parwani, A. V. (2013). Validating whole slide imaging for diagnostic purposes in pathology: Guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Archives of Pathology & Laboratory Medicine, 137(12), 1710–1722.
Shafi, S., & Parwani, A. V. (2023). Artificial intelligence in diagnostic pathology. Diagnostic Pathology, 18, Article 109. https://doi.org/10.1186/s13000-023-01375-z
U.S. Food and Drug Administration. (2021). Evaluation of automatic class III designation for Paige Prostate (DEN200080). https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN200080.pdf