

NYCAR Research Edition
Community Protection, Integrated Services, and Case-Based System Strengthening
Research Publication by Nancy O. Ugwu
Social Work and Health Care Services in Africa
NYCAR Research Publication | June 2026
Publication No.: NYCAR-TTR-2026-RP060
DOI: https://doi.org/10.5281/zenodo.20631815
Peer Review and Publication Status:
This research publication has passed NYCAR’s internal peer review for the June 2026 Research Edition. The review examined the strength of the central problem, the coherence of the chapter structure, the professional handling of social work within African health systems, the quality of the case analysis, the use of current public evidence, APA 7th citation discipline, figure presentation, and the practical value of the recommendations for health and social care administration.
The reviewer found the work suitable for public release because it treats social work as a serious health-system function rather than as a charitable afterthought. The publication shows master’s-level judgment, keeps the country cases distinct, connects evidence to practice, and offers a service model that can inform professional discussion, institutional planning, and policy-facing research. NYCAR approves this work as a publication-ready academic and professional research output.
Copyright © June 2026 Nancy O. Ugwu. All rights reserved. New York Center for Advanced Research (NYCAR).
Table of Contents
Abstract
Illness in African health systems often becomes most dangerous after the patient has already been seen. The consultation may be competent, the medicine appropriate, and the advice clear, yet the patient returns to conditions that make the plan almost impossible to follow. Transport money may be absent. Food may be uncertain. A woman may be unsafe at home. A child may depend on a caregiver already stretched beyond capacity. A person living with HIV, tuberculosis, diabetes, disability, depression, or chronic pain may understand the treatment plan but lack privacy, income, family support, or a reliable route back to care. The weakness, in such cases, is not simply medical. It is the failure of the service to stay connected to the life into which care is released.
Nancy O. Ugwu’s research publication places social work at that point of failure and possibility. It argues for social work as a health-system function with defined responsibility for social-risk assessment, safeguarding, referral follow-up, welfare linkage, family support, case recording, and continuity after the clinic visit.
The study uses Rwanda, Ghana, Kenya, and South Africa as focused country cases. Rwanda is read through community follow-up and the burden placed on local health workers. Ghana brings forward the limits of health financing when household costs, documents, distance, and informal barriers still decide access. Kenya raises the administrative question of how community health promoters, county systems, and digital reporting can improve care without turning frontline workers into unsupported carriers of system failure. South Africa shows the heavier intersection of HIV, TB, mental health, stigma, poverty, violence, and rights protection, where clinical treatment and social protection cannot be separated in the patient’s actual journey.
The publication advances a practical service model for African health care. Its standard is simple: once a health worker has seen that poverty, stigma, violence, disability, neglect, household instability, or welfare exclusion is threatening care, that knowledge must not die in conversation. It must enter a responsible pathway, with consent, confidentiality, a named worker, a referral destination, supervision, and follow-up. Social work strengthens health care when it prevents vulnerable patients from becoming their own case managers at the exact moment when illness has made them least able to carry that burden.
Keywords: Social work; health care services; Africa; community health; social protection; case management; primary health care; Rwanda; Ghana; Kenya; South Africa; referral completion; health administration.
Chapter 1: Social Work, Health Care, and the Household Reality of Illness in Africa
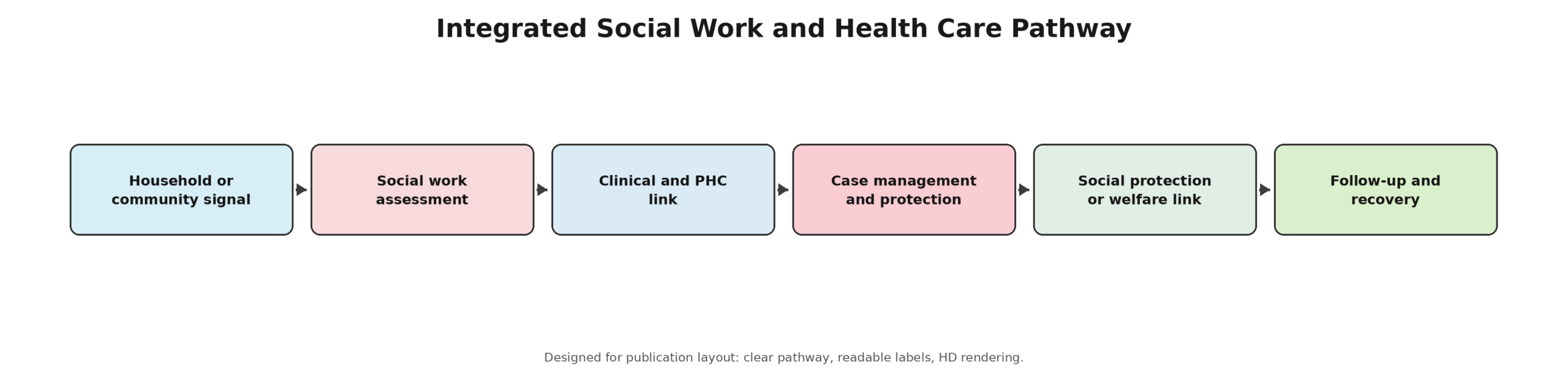
Figure 1. Integrated social work and health care pathway. Source: Author synthesis from WHO AFRO, UNICEF, World Bank, and case-study literature. Copyright © June 2026 NYCAR and Nancy O. Ugwu. All rights reserved.
Across Africa, the clinic visit is only one part of the story of care. A woman may reach an antenatal clinic after borrowing transport money, hiding a pregnancy from a violent partner, or leaving farm work during a season when each day of labor matters. A child with repeated infection may be treated correctly and sent home to unsafe water, little food, or a caregiver too exhausted to complete follow-up. A man on long-term treatment for HIV, diabetes, tuberculosis, or hypertension may know the instructions but lack privacy, stable income, transport, or family support. In each case the medical plan is shaped by social conditions that are visible to workers but often absent from formal records. Health administration that ignores those conditions is unlikely to protect patients well. Facility managers can count consultations, medicines, beds, clinic registers, and attendance, yet the more difficult question is whether the patient can act on what the service gives. When the barriers sit outside the consultation room, a narrow clinical file leaves the system partly blind. Social work helps close that blindness. It gives health services a disciplined way to assess household risk, protect rights, identify harm, arrange support, and check whether a referral reached its destination.
In this field, social work is part of health-system capacity, not sympathy at the edge of medicine. Social workers, welfare officers, community case managers, trained community health personnel, and patient-support teams can help health services remain connected to the lived conditions that decide whether care continues. That contribution is strongest where the patient faces several risks at once: poverty and pregnancy, disability and transport barriers, HIV and stigma, mental distress and unemployment, violence and child health, chronic illness and caregiving strain.
Recent public evidence gives the subject urgency. WHO AFRO reported that the African Region had an estimated 5.72 million health workers in 2024, while community health workers represented about 1.15 million of that reported workforce. The same regional evidence still projected a shortage of 5.85 million health workers by 2030 (WHO AFRO, 2026). Such figures do not mean that social workers can replace clinicians. They show why health systems need every practical role to be clearly designed, supervised, and connected to the places where patients live. Public social-protection evidence points in the same direction. UNICEF, ILO, and Save the Children reported in 2024 that 1.4 billion children aged 0 to 15 had no form of social protection, while fewer than one in ten children in low-income countries had access to child benefits (UNICEF, 2024). That finding matters for health because children without income support are often the same children whose families delay care, miss school, lack food, or struggle to complete treatment. Health care cannot solve social poverty by itself, but it must know when poverty is defeating care.
At master’s level, the subject requires more than a moral appeal. The research question is how the profession can be placed inside health care services in a way that is professional, accountable, measurable, and respectful of African country differences. It asks what social work contributes to primary care, community health, financing access, HIV and TB support, mental-health integration, discharge safety, and protection for children, older people, persons with disabilities, survivors of violence, and households under financial stress. Four country cases carry the analysis. Rwanda is used to examine community health and household continuity because its community health worker experience shows both the reach and burden of community-based care. Ghana is used to examine health financing and household protection because insurance or public spending reforms can still leave vulnerable families unable to use care. Kenya is used to examine community health promoters, county service design, and digital records. South Africa is used to examine HIV, TB, mental health, stigma, and integrated support in a high-burden setting.
These cases are not offered as a continental template. Africa is not one health system. Law, financing, disease burden, public administration, conflict history, welfare capacity, languages, family structure, and civil-society strength differ by country and within countries. Comparison is valuable only when it respects difference. Rwanda may demonstrate disciplined community reach, but a rural district elsewhere may lack the financing or supervisory structure to copy it. Kenya may legislate community health reform, but counties vary in capacity. Ghana may expand financing arrangements, yet indirect household costs remain. South Africa may have mature HIV infrastructure while still carrying stigma, mental-health burden, and inequality. The research design is a public-evidence case study. It draws from WHO AFRO, UNICEF, the World Bank, Kenyan policy material, South African HIV and TB strategy, and peer-reviewed studies on community health, gender-transformative prevention, and mental-health integration.
It does not invent interviews, field observations, patient datasets, or unpublished government figures. Where quantitative data appear, they are presented as public indicators rather than original statistical findings. That restraint matters because health-service writing must separate evidence from opinion, especially when vulnerable households are used to explain institutional failure. Its contribution is practical. It identifies the point at which a clinical system should hand off to social-work response, how consent and confidentiality should be handled, why referral completion must be measured, and how health administrators can avoid using community workers as unpaid shock absorbers for gaps in formal services. It also argues that social work should not be placed in health care as decoration. Role clarity, supervision, case records, referral authority, worker protection, and outcome review are the conditions that turn social concern into service reliability.
A final concern shapes the whole study: dignity. Vulnerable patients should not have to master the boundaries between health, welfare, education, justice, local government, and charities while facing illness. When agencies fail to coordinate, the patient becomes the messenger and the poorest household pays the highest price. Social work helps a health system remember the whole person after the prescription, discharge note, referral slip, or clinic card has been issued. That memory is a form of care. The discussion moves from the health-social interface to the four country cases, and then to an African social work-health service model that administrators can adapt. The writing avoids a sentimental view of social work. It also rejects the idea that clinical services alone can carry the full burden of illness. Health care becomes safer when the system sees the person’s social world early enough to act. That is the standard used throughout this publication. Publication writing also requires care not to pretend that all African settings have the same administrative capacity. A district hospital in northern Ghana, a county clinic in Kenya, a community health post in Rwanda, and an HIV service in South Africa may all face social risk, but the route to solve it will differ.
The common standard is not identical structure. It is the refusal to leave patients alone with problems that the service has already seen. Health leaders often speak of integration after services fail. The discussion treats integration as preparation. If a clinic knows that poor patients miss follow-up because transport costs are high, that knowledge should shape the referral pathway before the next patient is lost. If a community worker sees repeated family violence, the service should not wait for a tragedy before building a protection route. Good administration learns before harm repeats. African health administration also needs a stronger language for the space between diagnosis and recovery. The patient leaves with medicine, but the household may have no food, no privacy, no transport, or no safe person to help.
A paper record may show that care was delivered, while daily life shows that care was never truly usable. Social work gives managers a way to examine that gap without blaming the patient for conditions created by poverty, stigma, or weak coordination. A master’s-level reading of the subject must also separate advocacy from service architecture. Advocacy names the moral duty to protect people. Service architecture names the routes, staffing, records, referral points, and review meetings that make protection happen. African health systems need both. Without advocacy, the subject loses urgency. Without architecture, the language of concern becomes another promise that frontline workers cannot deliver. Each country case is used for a different administrative reason. Rwanda clarifies community continuity. Ghana tests whether financial protection is usable at household level. Kenya shows what formalized community work and digital records can add when counties have real support. South Africa exposes the link between HIV, TB, mental health, stigma, and rights-based care. Read together, the cases do not flatten Africa into one model; they show how social-work judgment must be adapted to the place where care is actually delivered.
Public health and social welfare are often planned through separate budgets, but patients do not live inside budget categories. A child with untreated illness may need school contact, food support, water safety, and caregiver help. A mother may need antenatal care and protection from violence. A person with HIV may need medicine and protection from disclosure harm. The health outcome depends on more than the clinical contact.
Chapter 2: Social Work as Health-System Capacity, Not Charity
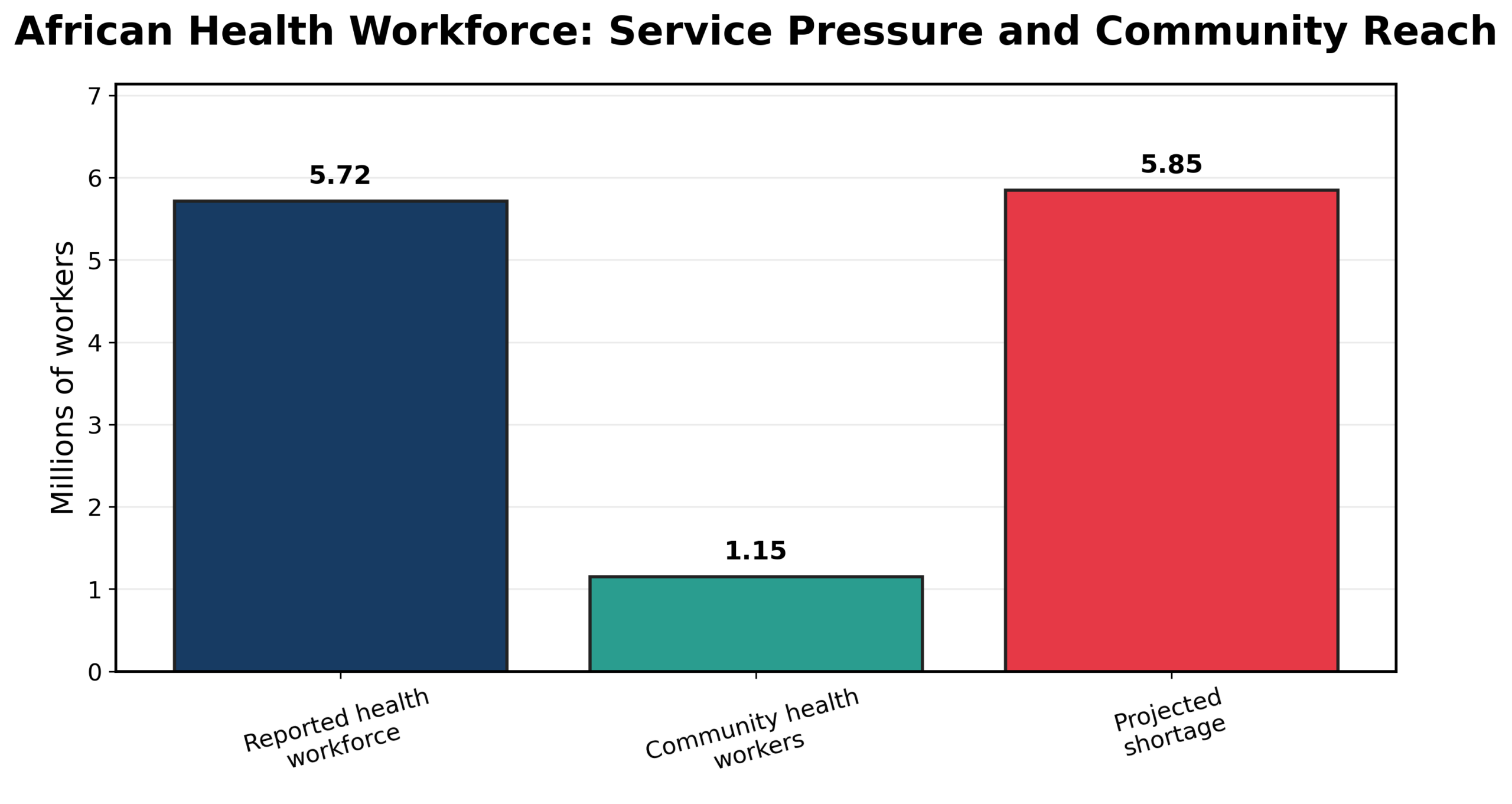
Figure 2. African health workforce pressure and community reach. Source: WHO AFRO (2026). Copyright © June 2026 NYCAR and Nancy O. Ugwu. All rights reserved.
Social work belongs in health care because illness rarely arrives alone. A patient with chest pain may also be a wage earner whose absence means lost food at home. A child with malnutrition may live in a household where the caregiver has no income, no safe water, and no reliable transport. A survivor of violence may come to a clinic for wound care while fearing what will happen after disclosure. Clinical treatment may be correct, yet care remains fragile if the service has no route for the risks surrounding the patient. A health service that includes social work is better able to ask what has to happen around the patient for treatment to hold. That question moves the discussion away from charity and toward service design. It asks who will assess risk, where the file will be recorded, who owns the referral, how consent will be obtained, what support exists, and how the system will know whether the patient actually received help. These are administrative questions with direct health consequences.
Primary health care gives the strongest entry point. Local clinics, maternal services, immunization contacts, child-health checks, chronic-disease reviews, HIV and TB services, emergency units, mental-health touchpoints, and discharge planning all reveal social risk. A missed appointment may signal poverty, stigma, disability, partner control, transport failure, or distrust. Without a social-work response, staff may record nonattendance and move on. With a case route, the service can ask why the patient did not return and whether a preventable barrier can be removed.
Table 1. Public Evidence Base Used in the Study
| Evidence area | Source base | Use in the paper |
| Health workforce | WHO AFRO (2026) | Frames workforce pressure, community health worker reach, and the need for role clarity. |
| Child and household protection | UNICEF, ILO, and Save the Children (2024); UNICEF Ghana (2024) | Links health care with poverty, child vulnerability, and social protection gaps. |
| Community health | Hezagira et al. (2025); Ministry of Health Kenya (2020); PATH (2023) | Supports Rwanda and Kenya case analysis on community delivery and formalization. |
| Health financing | World Bank (2024); World Bank Open Knowledge (2024) | Supports Ghana case analysis on UHC, household costs, and financing limits. |
| HIV, TB, and mental health | SANAC (2023); UNAIDS (2025); Regenauer et al. (2024); Adjorlolo et al. (2025) | Supports South Africa case analysis on integrated care, stigma, and psychosocial support. |
Workforce pressure makes the role more urgent. WHO AFRO’s 2026 workforce evidence shows growth in the region’s health workforce and strong presence of community health workers, yet the projected 2030 shortage remains severe (WHO AFRO, 2026). In that environment, role confusion becomes costly. Nurses, doctors, and community health workers cannot safely absorb every welfare, protection, transport, family, and mental-health problem that appears in clinical practice. Social workers cannot replace them either. Each group needs a defined place in a joined pathway. Case management is one of the clearest ways social work adds value. A case manager identifies the problem, assesses risk, ranks urgency, seeks consent, arranges referral, documents action, and returns to the file. This process may sound basic, but many patients fall through gaps because no one owns the movement between services. A referral slip without a named destination, timeframe, and feedback loop is often advice rather than service. Social work turns referral into a managed responsibility. Safeguarding provides another reason for integration. Children, persons with disabilities, older adults, survivors of gender-based violence, migrants, and people living with mental illness may face harm that clinicians notice but cannot manage alone.
A child who returns repeatedly with injuries, a pregnant adolescent afraid to speak, an older patient abandoned after discharge, or a patient with HIV facing family rejection needs more than medical treatment. Trained social-work response helps the system act without improvisation, panic, or unsafe disclosure. Ethics must sit at the core of any health-social model. Social work in clinics and communities involves private information about violence, HIV status, pregnancy, mental health, poverty, disability, child protection, immigration, substance use, and family conflict. Poorly handled information can expose people to stigma, retaliation, shame, job loss, or renewed violence. Integration should never mean casual sharing. It requires consent rules, limited access, secure records, and supervision that teaches workers what to document, what to protect, and when safety overrides ordinary confidentiality.
Social determinants of health are often discussed in policy language. Social work translates that language into practice. If food, housing, income, violence, discrimination, education, water, employment, and caregiving shape health, a health service needs people who can assess those conditions and link patients to support. Otherwise, reports may speak about determinants while clinics continue to treat only their consequences. The profession’s practical value lies in connecting assessment with action. Health financing also needs a social-work lens. Insurance or public financing may reduce direct fees, but families still face transport, lost wages, medicines outside benefit packages, informal costs, caregiving time, and documents required for enrollment or renewal. Patient navigation helps vulnerable households understand entitlements, use benefits, and remain connected to care. A financing reform that looks strong in policy may still fail poor households if no one helps them cross the administrative distance between eligibility and real access.
Community health workers are often closest to household realities. They may see the food shortage, the missed medication, the unsafe sleeping arrangement, the child not in school, the family conflict, or the person hiding treatment. Their closeness is valuable, but it can also be risky if they lack training and backup. Social-work partnership gives community work a safer route for cases that require protection, counseling, welfare linkage, or mental-health referral. It also protects community workers from being asked to solve problems outside their role. Administrators benefit because social-work records can reveal patterns. Repeated missed appointments may point to transport gaps. Treatment interruption may point to food insecurity. Unsafe discharge may point to absence of caregiver assessment.
Child health problems may point to welfare delays or protection failure. When case notes are anonymized and reviewed responsibly, individual hardship becomes system learning. The evidence can guide service redesign without turning patients into data points stripped of dignity. A mature health-social system also protects workers. Social workers and community personnel deal with grief, hunger, violence, untreated illness, family conflict, and state failure at close range. Praising their compassion while denying supervision, safe caseloads, transport, and psychological support is poor management. Worker protection is not a luxury; it is quality control. Staff who are overwhelmed or unsupported cannot provide careful, ethical, steady follow-up. The conceptual point is simple but demanding: social work in health care should be designed as a service function with authority and limits. It should not be a vague appeal to caring behavior. It should have referral criteria, forms that do not overcollect private details, supervision arrangements, links to welfare and protection agencies, and measures of completion. Patients deserve care that does not stop at the edge of a professional boundary. Social work also guards against a narrow idea of efficiency. A clinic may appear efficient when it moves patients quickly, but speed without resolution can produce repeated use, avoidable deterioration, and hidden family burden. A slower social-risk review at the right moment may prevent a more expensive crisis later. Managers should treat that review as part of safe throughput, not as a delay.
Professional boundaries remain necessary. Social workers should not diagnose diseases or prescribe medicines. Clinicians should not be expected to settle welfare eligibility or child-protection cases alone. Community health workers should not be asked to carry confidential trauma without supervision. Integration works when each profession knows its task and respects the tasks of others. A serious social-work role also reduces waste. Repeated crisis visits, abandoned treatment, failed discharge, and late presentation carry financial cost as well as human cost. When a worker identifies the transport barrier, the unsafe home, the food gap, or the fear that keeps a patient away, the service receives information that can prevent repeated use. That is health management, not sentiment. Professional education should reflect this reality. Social workers entering health settings need knowledge of clinical pathways, public-health aims, and referral urgency. Health workers need enough understanding of social risk to know when to ask for help. Joint learning prevents two common failures: clinicians ignoring social harm because it is outside their training, and social workers underestimating clinical risk because the social story is so demanding.
Chapter 3: Rwanda, Community Health, and the Discipline of Household Follow-Up
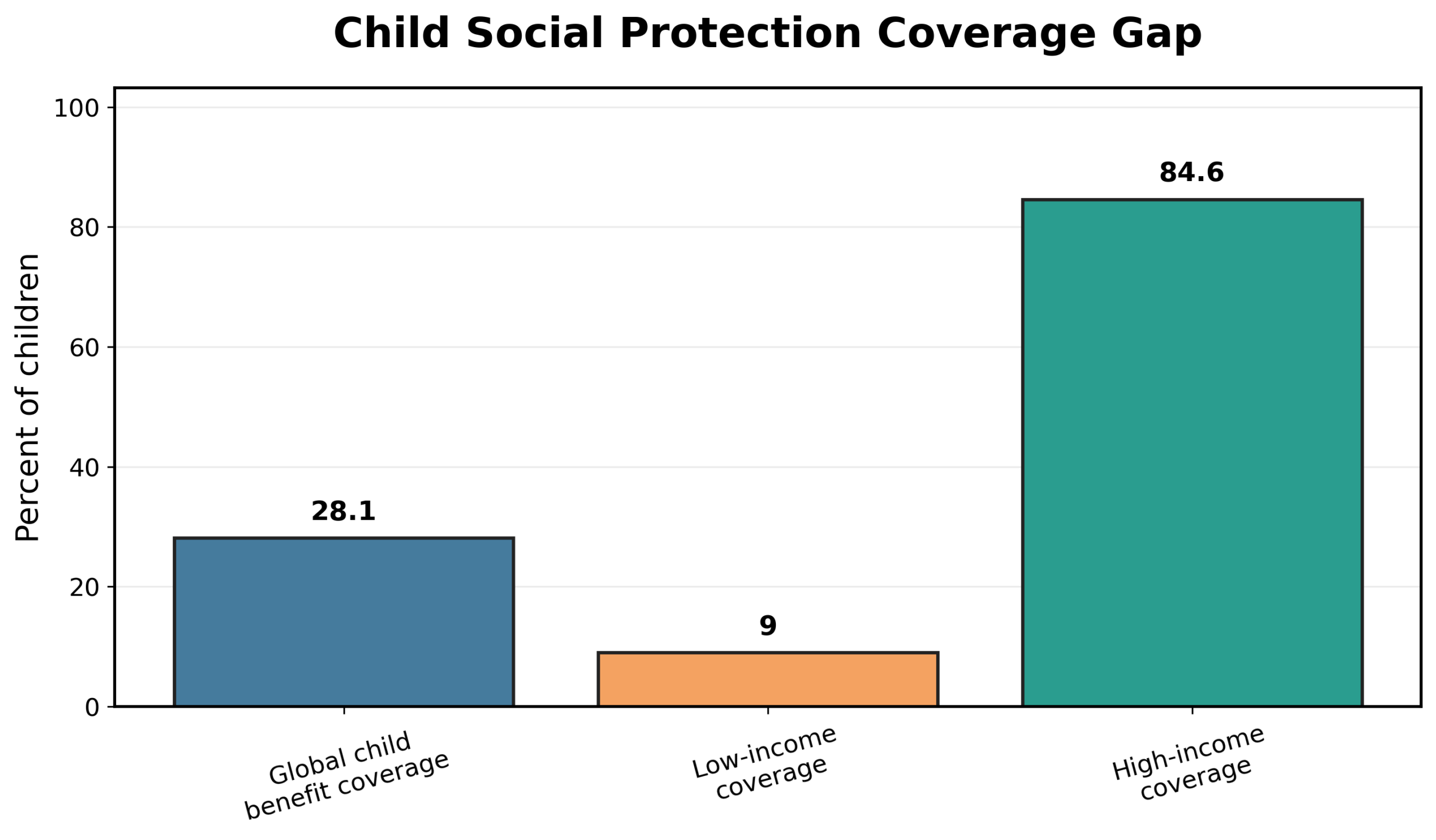
Figure 3. Child and household protection signals. Source: UNICEF (2024) and author analytical synthesis. Copyright © June 2026 NYCAR and Nancy O. Ugwu. All rights reserved.
Rwanda is valuable here because community health has been treated as a serious part of national health strategy rather than a temporary volunteer add-on. Recent peer-reviewed work on three decades of community health workers in Rwanda describes a system that has evolved through policy design, training, expansion, and adaptation (Hezagira et al., 2025). The relevance for social work lies in the place where community health workers stand: close enough to see household risk, but often without the professional authority or resources to manage every problem they encounter. Community health workers can support maternal and child health, prevention, screening, treatment literacy, referral, and follow-up. They know pathways to homes, local leaders, family pressures, and the ordinary reasons people delay care. That knowledge gives the health system reach. It also creates ethical exposure. A worker may learn about violence, hunger, treatment interruption, mental distress, disability neglect, or a child not attending school. Without a safe referral route, the worker can be left with information that is too serious for informal advice.
Social work strengthens the Rwandan community-health lesson by giving household risk a professional response. A community worker who identifies a problem should know whether the file requires health education, clinical referral, welfare support, child protection, counseling, or urgent safeguarding. That distinction is not always obvious. A missed maternal appointment may mean transport hardship, partner control, fear, misinformation, illness, or neglect. Social work helps the system examine the household setting before labeling the patient as noncompliant.
Table 2. Rwanda Case Lessons for Health-Related Social Work
| Observed issue | Social-work implication | Management action |
| Community proximity | Workers see household risk early, including violence, poverty, and missed care. | Create escalation routes to social workers, welfare offices, and protection teams. |
| Trust and confidentiality | Local knowledge can protect care or expose families if mishandled. | Train workers in consent, safe records, and limits of disclosure. |
| Referral feedback | A referral without feedback leaves community workers without authority. | Require referral completion review and case-return notes. |
| Worker burden | Frontline roles carry emotional and ethical load. | Provide supervision, transport support, and role boundaries. |
Rwanda also shows why community legitimacy must be protected. A trusted local worker can enter spaces that a distant official may never reach. Yet trust can be damaged quickly if private information becomes gossip, if referrals lead nowhere, or if promises are made beyond the service’s capacity. Training should cover confidentiality, respectful communication, consent, and honest explanation of what can and cannot be provided. Community proximity is an asset only when the system uses it responsibly. The Bandebereho experience adds a useful social-protection dimension. Research on equipping community health workers in Rwanda to deliver a violence-prevention parenting program links community platforms with prevention of violence against women and children (Doyle et al., 2025). That does not mean every community health worker should become a specialist in family violence. It means that health-adjacent programs can identify social harm when training, supervision, referral, and role limits are handled carefully.
For social work, the lesson is that health outreach and social protection can meet in the same household. A visit for child health may reveal harsh discipline, caregiver stress, food insecurity, or an unsafe relationship. A maternal-health contact may reveal partner control or lack of transport. A chronic-care follow-up may reveal depression or stigma. The practical question is whether the system has a route for action. Seeing risk without response creates frustration and potential harm.
Records matter in this case. Community contact has little long-term value if the system cannot remember what was seen, what was agreed, and who will follow up. A simple protected case note can help a clinic, welfare office, or social worker know what has happened. Poor records force patients to repeat private stories and make workers depend on memory. Good records protect continuity while limiting sensitive details to what is needed for care. Supervision is another management issue. Community workers who repeatedly encounter poverty, death, violence, and untreated illness carry emotional burden. Celebrating them in policy speeches does not reduce that burden. A social-work layer can provide case consultation, escalation, and reflective support. That function helps workers know when to continue routine follow-up, when to ask for clinical review, and when a case has crossed into protection or mental-health territory. Rwanda’s case also warns against copying without context. Community health is strong when policy, community trust, financing, training, supervision, supplies, and referral routes align. Removing one part weakens the rest. A country that copies household visits without paying attention to supervision may expand contact but not quality.
A district that trains workers without creating referral feedback may increase reporting but leave patients in the same danger. Reform has to be carried by real capacity. Another lesson concerns the difference between outreach and continuity. Campaigns can find people. Continuity keeps them connected. Many systems are better at reaching households during a program cycle than staying with a case until risk has reduced. Social work pushes health services toward continuity because it asks whether the family reached support, whether the child remained safe, whether the appointment was kept, whether the welfare link worked, and whether new risk appeared. In practice, Rwanda suggests that social work should not be added to community health after problems pile up.
It should be built into the design from the start. Community workers need a map of social services, a channel to social workers or welfare officers, a safe way to record risk, and feedback when referrals are completed. Social workers need to understand community health workflows so they do not create unrealistic paperwork or delays. Both sides need shared language. The Rwandan example supports a wider African lesson: local presence is powerful, but it is not enough. A trusted community worker can notice hardship early, yet a patient benefits only when the system can respond. Professional social work gives that response structure. It turns household knowledge into assessment, protection, referral, and follow-up. Without that structure, community health may become a heavy moral burden placed on workers who are close to suffering but far from decision-making power. A well-run Rwandan-style community pathway would also make space for feedback from workers. People closest to households often understand why a policy fails in practice. They know which families cannot afford transport, which messages are misunderstood, which referral points are closed, and where stigma keeps people silent. Administrators lose intelligence when they treat frontline reports as anecdote rather than service evidence.
The same principle applies to household-level prevention. A community worker may notice early warning signs before a formal emergency exists. Food stress, missed medicines, social isolation, and school absence may appear small separately but dangerous in combination. Social-work supervision can help rank such risks and decide which cases need immediate action. The Rwandan case also has value for emergency readiness. Epidemics, floods, displacement, or local insecurity can quickly interrupt routine services. Community workers often become the link between households and formal response. If social-work logic is part of the system, emergency response can include protection, family tracing, disability support, mental-health referral, and help for isolated households rather than only disease messages.
Household continuity should also be treated as a quality measure. A patient reached once is not necessarily protected. Care becomes stronger when the same case is followed long enough to know whether the risk declined. In maternal health, that may mean confirming return visits. In child protection, it may mean checking safety. In chronic care, it may mean knowing whether medication, food, and transport are stable enough for treatment to continue. Rwanda also shows why community systems need honest workload assessment. A household may present several needs during one visit: immunization, malnutrition, domestic conflict, poverty, and a missed appointment. If the worker has no time, phone credit, transport, or referral contact, the system has created a role that sees risk but cannot act. That gap is professionally unsafe. Social-work supervision can give such workers a place to bring uncertainty. Is a case urgent? Is consent needed before calling another office? Is the child unsafe? Is the patient refusing care or unable to reach care? These are judgment questions. Community systems become more reliable when workers are not forced to answer them alone.
Chapter 4: Ghana, Health Financing, and Household Protection
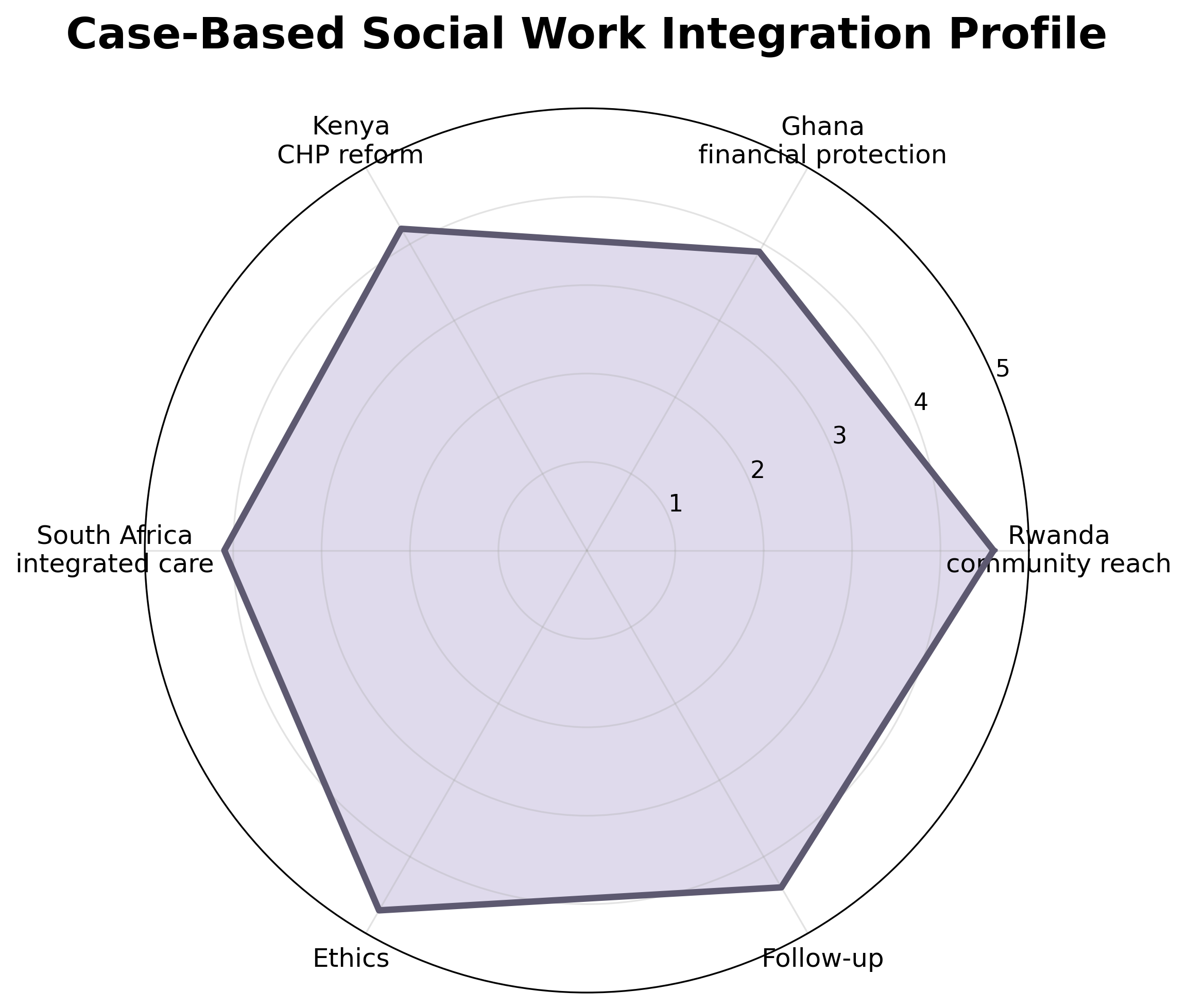
Figure 4. Case-based integration profile. Source: Author analytical model from Rwanda, Ghana, Kenya, and South Africa evidence. Copyright © June 2026 NYCAR and Nancy O. Ugwu. All rights reserved.
Ghana is valuable because it shows how health financing and social work meet at household level. Insurance and public spending reforms can reduce barriers, but they do not remove every cost that families face. Transport, food, lost work time, caregiver absence, informal payments, medicine gaps, documents, and renewal procedures can still decide whether a patient receives care. A financing system may look organized from Accra and still feel difficult in a rural household or informal settlement. World Bank work on public health expenditure for universal health coverage in Ghana notes the country’s progress while also pointing to financing challenges and the role of public funding through the Ministry of Health and National Health Insurance Scheme (World Bank, 2024). For social work, the key issue is how those financing arrangements are experienced by people with weak bargaining power: children, persons with disabilities, women exposed to partner control, older people, migrants, and families whose income collapses during illness.
Ghana’s National Health Insurance Scheme has long attracted attention because it represents an African attempt to institutionalize financial protection. Yet coverage is not the same as usable care. A family may be registered but still unable to travel. A patient may have a card but lack money for food during treatment. A caregiver may not understand renewal rules. An older person may be covered for a consultation but not for the full cost of recovery. Social work helps identify the difference between legal entitlement and practical access.
Table 3. Ghana Case: From Financial Coverage to Household Use
| Policy issue | Household barrier | Social-work contribution |
| Insurance enrollment | Documents, renewal, travel, unclear benefits | Patient navigation and eligibility support. |
| Indirect cost | Transport, food, lost work time, caregiver burden | Household assessment and welfare linkage. |
| Child protection | Children outside effective coverage or social support | Referral to child welfare, school, and family support. |
| Chronic illness | Repeated costs and treatment fatigue | Case planning, adherence support, and early crisis prevention. |
Children make that difference visible. UNICEF Ghana’s social-protection material has discussed children who remain outside key protection arrangements and the connection between household vulnerability and service access (UNICEF Ghana, 2024). A child without effective protection may miss treatment because a caregiver cannot pay indirect costs, lacks documents, lives far from services, or does not know how to use available support. Health care and welfare policy meet in that child’s case, even if ministries file them separately.
A social-work role in health financing is partly navigational. Many households need help understanding what benefits exist, what documents are required, which service is covered, where to renew, and how to appeal or ask for assistance. Navigation is not a minor convenience for families with limited literacy, mobility, time, or confidence in institutions. It can decide whether a benefit becomes actual care. Patient support workers, social workers, and trained welfare officers can convert policy language into action. Financial protection also concerns chronic disease. Diabetes, kidney disease, cancer, hypertension, HIV, mental illness, and disability can create repeated costs. A single clinic visit may be affordable while the long sequence of tests, medicines, transport, diet changes, and caregiving becomes unbearable. Social work helps by assessing household strain early, connecting families to available welfare support, and helping health managers see when repeated indirect costs are driving treatment interruption.
Ghana’s case also raises the issue of administrative simplicity. Rules that look orderly to policymakers may be burdensome for poor families. A benefit that requires several visits, forms, fees, or identification documents can exclude the people it was meant to support. Social workers see these barriers because they sit close to patients. Their records should feed back into policy review. When many patients miss care because renewal is difficult or transport is unaffordable, that is not individual failure; it is administrative evidence.
Household protection should be read widely. Money matters, but protection also includes safety, caregiving, child welfare, disability support, legal identity, nutrition, school continuity, and shelter. A woman receiving maternal care may need protection from violence more urgently than a benefit leaflet. A child with epilepsy may need school support and caregiver education. A person with disability may need accessible transport and assistive devices. Social work keeps these linked needs visible to health services. The Ghana case strengthens the argument that financing reform and social care should be planned together. Health ministries cannot treat household hardship as a separate policy universe when hardship decides whether care is used. Welfare agencies cannot protect families fully when health costs and illness push households into crisis. Coordination does not require every agency to merge. It requires clear referral points, shared eligibility knowledge, and review of whether assistance reached the person. Data can improve the connection. Clinics should not simply record that a patient missed an appointment. They should ask whether the barrier involved cost, distance, family control, medication availability, work pressure, fear, or misunderstanding. Aggregated responsibly, that information can show where financing reform is not translating into access. Social workers and patient navigators are well placed to gather this information without blaming patients for structural barriers.
Ghana also shows why social work must avoid making promises that the state cannot keep. If benefits are limited, staff should be honest. If a referral is unlikely to result in immediate support, patients should know. Ethical practice requires candor because desperate households can be harmed by false assurance. At the same time, even limited support can matter when directed carefully. Knowing what exists and how to reach it is part of service quality. Ghana’s lesson is that financial protection becomes real only when households can use it. Insurance, budget allocation, and UHC targets are necessary but incomplete. Social work makes the household economy visible. It can help a health system distinguish refusal from hardship, delay from fear, and nonattendance from administrative exclusion. That is why social work belongs in health financing discussions, not merely in welfare offices after care has already failed.
Health financing reform can also affect trust. When patients are told that care is covered but later face unexpected costs, confidence weakens. Social workers and navigators often become the people who hear these complaints. Their feedback can help managers identify whether the problem is benefit design, poor communication, supply gaps, or informal charges. Ignoring such feedback allows distrust to grow. Ghana’s case also underlines the place of families. Illness changes household budgets, gender roles, children’s schooling, and caregiving expectations. A patient may choose between treatment and food, or a caregiver may stop working to accompany someone to appointments. Social work makes these choices visible and helps the health service understand the cost of care beyond the facility wall. Ghana also shows why household data should be used carefully. A family’s inability to pay should never become a mark of shame in a clinical record. The purpose of recording financial strain is to link support and improve service design. Managers should review patterns without exposing individual households. Dignity in data handling is part of financial protection.
Another lesson from Ghana is that welfare and health workers need shared understanding of eligibility. A clinic that sees need may not know whether a patient qualifies for assistance. A welfare office may not understand the urgency created by a medical condition. Regular liaison can reduce this gap. Even where resources are scarce, coordination can prevent avoidable delay and repeated confusion. That shared understanding turns eligibility from a paper rule into an actual route through which vulnerable households can keep care within reach.
Chapter 5: Kenya, Community Health Promoters, and Digital Accountability
Kenya offers a current case because its recent legal and policy agenda has sought to formalize community health and rework financing and digital systems. PATH’s 2023 overview describes the Social Health Insurance Act, Primary Health Care Act, Digital Health Act, and the place of community health promoters in the reform package (PATH, 2023). This case is useful because it shows a country trying to move community delivery from informal contribution toward recognized service architecture. Kenya’s National Community Health Strategy 2020-2025 placed community health at the foundation of universal health coverage and linked community units with primary care delivery (Ministry of Health Kenya, 2020). That orientation matters for social work. Community health promoters can support prevention, treatment literacy, referral, maternal and child health, public-health messaging, and household continuity. Yet household contact also exposes them to social problems that sit beyond routine health education. A community health promoter may be the person who learns that a pregnant woman is being controlled by a partner, that a child with disability is hidden at home, that a patient with tuberculosis fears stigma, or that an older person has no one to help with daily care. Those findings cannot be managed through slogans. They need a structured route to social-work assessment, welfare support, child protection, mental-health referral, or clinical review. Social work gives community health reform a safer case pathway.
Table 4. Kenya Case: Community Health Promoters and Social-Work Interfaces
| Reform area | Risk if poorly designed | Required social-work link |
| Community health promotion | Expanded tasks without referral authority | Clear escalation to welfare, protection, and clinical teams. |
| Digital health | Sensitive household data exposed or misused | Consent, privacy rules, access controls, and worker training. |
| County delivery | Uneven capacity across counties | Minimum national standards with local adaptation. |
| Health financing reform | Registration without actual service use | Patient navigation and household follow-up. |
Formalization can improve community health when it brings training, supervision, payment or incentives, supplies, data tools, and accountability. It can also create new burdens if tasks multiply faster than support. A title alone does not make a role safe. Community health promoters need clear limits. Social workers need clear criteria for when a household case should be transferred or jointly managed. Health administrators need to know which problems are being referred repeatedly and why. Kenya’s county structure adds another layer. Demainization can help services respond to local geography, languages, and community organizations. It can also produce unequal capacity. Some counties may support community health better than others. A national model for social work-health integration should allow local adaptation while keeping minimum standards for supervision, referral, confidentiality, and case completion. A household should not lose protection because local administration is weaker. Digital health reform deserves close attention. Digital records, dashboards, unique identification, and reporting systems can improve continuity if they are designed around care. They can also expose sensitive information. Community health promoters and social workers may hold details about HIV, pregnancy, violence, disability, mental distress, poverty, and family conflict. Digitizing such information without strict access controls and worker training can damage trust. Patients will not disclose risk if they fear public exposure.
A social-work lens makes the digital agenda more careful. It asks what information is truly needed, who can see it, how consent is recorded, how a patient can challenge errors, and what happens when a record signals danger. Data should help solve the problems communities report. If information travels upward but does not improve local support, workers may lose confidence and households may stop sharing.
Kenya’s case also clarifies what integration means in practice. It is not enough to place different workers in the same community. Integration requires referral forms that are easy to use, defined responsibilities, feedback routes, shared supervision meetings, and authority to solve problems. A promoter who identifies a household risk should know the referral destination. A social worker who receives the case should know how to speak with the clinic. The clinic should know whether the support happened. This professional role can also help with health literacy. Insurance changes, primary care reforms, digital enrollment, and referral pathways can confuse patients. Community-based workers may explain what has changed, but complicated household situations may require more focused support. A person with disability, a grandmother caring for orphaned children, a survivor of violence, or a migrant household may need someone who can connect health instructions with welfare, school, legal, and protection services.
Worker protection remains a serious concern. Community health promoters are often praised as the face of reform, but praise will not carry transport costs, safety risks, emotional load, or household expectations. Social-work partnership should not become another way to shift responsibility downward. Both promoters and social workers need manageable caseloads, supervision, safe reporting procedures, supplies, and realistic referral options. Reform that overloads frontline staff weakens its own credibility.
Measurement should focus on completion, not merely contact. How many households were visited? That question has value, but it is insufficient. Better questions are whether the referred patient reached the clinic, whether the abused person received protection support, whether the child returned to care, whether a missed appointment was followed up, and whether the social barrier was reduced. Community health becomes stronger when contact is linked to outcome. Kenya’s lesson for African systems is that formal community health reform should be designed with social risk in mind from the beginning. When legal, digital, and financing reforms move faster than household support, vulnerable people may remain outside the care promise. Social work helps keep the reform anchored in the lives of people who use services. It asks the system to pay attention not just to who was registered, but to who was reached, protected, and followed until help became real. A careful Kenyan model would also protect communities from data fatigue. Households may be asked to provide information repeatedly to different workers and programs. If nothing improves after disclosure, people become less willing to speak honestly. Social-work practice insists that questions should have purpose. A service should ask because it intends to act, not because a dashboard demands another field.
County managers can use social-work reports to compare local barriers. One county may see transport as the main barrier to follow-up, another may see fear of costs, another may see domestic violence or disability exclusion. A national policy cannot know every local pattern in advance. Local social-work evidence helps reform stay grounded. Kenya’s reform space also raises a professional question about digital identity. Linking a person to services can improve continuity, but it can also create fear among people who already distrust institutions. Patients need to know that information collected for care will not be used to punish, expose, or exclude them. Social-work ethics can help keep digital reform tied to trust. Community health promoters can also become a source of local learning. When many households report the same barrier, the problem belongs on a management agenda.
If mothers miss appointments because of transport, if disability referrals fail because offices are distant, or if adolescents avoid care because privacy is weak, those patterns should shape county planning. A good reform listens downward as well as reporting upward. Kenya’s digital agenda also raises a question about accountability to communities. If households provide data, they should see some benefit from the exchange. Better follow-up, clearer referrals, less repeated questioning, and quicker recognition of risk are practical signs that data serve care. When data flow only upward, communities may feel monitored rather than supported. Social workers can help interpret community data with caution. A high number of missed appointments in one area may indicate distance, staff behavior, insecurity, cost, stigma, or poor communication. Data show the pattern; local case knowledge explains it. Managers need both before making fair decisions.
Chapter 6: South Africa, HIV, TB, Mental Health, and Rights-Based Care
South Africa is a demanding case because HIV, tuberculosis, mental health, substance use, poverty, inequality, and stigma often appear in the same patient journey. A person may receive antiretroviral therapy while also facing depression, violence, unemployment, food insecurity, housing instability, or fear of disclosure. Health care that treats only the biomedical file can miss the social realities that shape adherence, retention, and safety. South Africa’s National Strategic Plan for HIV, TB and STIs 2023-2028 is explicitly multisectoral and people-centered (SANAC, 2023). That matters because HIV and TB are not merely clinical conditions. They are also shaped by social stigma, rights, employment, gender power, housing, mental health, substance use, and family relationships. A strong disease program still needs social-work capacity when patients are at risk of dropping out because the pressures around treatment are unmanaged.
UNAIDS reported that 40.8 million people were living with HIV globally in 2024, with eastern and southern Africa remaining one of the most affected regions (UNAIDS, 2025). South Africa carries one of the world’s largest HIV treatment responsibilities. Biomedical scale is vital, but scale alone does not eliminate fear, stigma, depression, gender-based violence, or treatment fatigue. Social work contributes by helping clinics understand why a patient disengages and what support may restore safe contact.
Table 5. South Africa Case: HIV, TB, Mental Health, and Social-Work Response
| Patient risk | Service weakness when untreated | Social-work response |
| Stigma and fear of disclosure | Avoided testing, hidden medication, missed visits | Disclosure planning, family support, rights counseling. |
| Depression or anxiety | Reduced adherence and treatment fatigue | Mental-health referral, psychosocial support, follow-up. |
| Substance use stigma | Judgment by workers and weak retention | Stigma-reduction support and linked care. |
| Violence or unsafe home | Treatment plan cannot be followed safely | Protection planning and confidential referral. |
Mental-health integration is especially relevant. Recent evidence on mental-health interventions for young people living with HIV in sub-Saharan Africa points to peer, family-based, and digital approaches while recognizing that the evidence base remains uneven (Adjorlolo et al., 2025). Another line of work in South Africa has examined community health worker training to reduce stigma around substance use and depression in HIV and TB care (Regenauer et al., 2024; Myers et al., 2024). These studies show that psychosocial issues are not side concerns. They influence whether treatment continues. This professional role can support integrated HIV and mental-health care through counseling, disclosure planning, family meetings, risk assessment, welfare referral, rights advice, and follow-up after missed visits. A patient who hides medication because of stigma may need a safer disclosure strategy.
A patient with depression may need mental-health referral and family support. A woman facing violence may need protection planning before treatment advice can be followed safely. These tasks require skill and confidentiality. Stigma operates as a health barrier because it changes behavior. People may avoid testing, conceal diagnosis, miss appointments, stop treatment, or refuse referral because they fear judgment. A clinical message alone may not overcome that fear. Social workers can help by working with support groups, families, community organizations, and clinic teams while protecting privacy. Rights-based care means that the patient’s dignity is protected while health services pursue disease control. Substance use presents another reason for joined care. Patients who use substances may be judged by workers, families, or communities. Stigma can reduce time spent with providers, weaken trust, and interrupt treatment. Training helps, but trained workers still need somewhere to send patients for support. A screening tool without counseling, harm-reduction referral, or social support becomes another form of exposure without help. Integration requires response capacity.
Gender-based violence also intersects with HIV and health care. Disclosure may be unsafe in some relationships. Partner control may restrict clinic attendance or medication use. A woman may present with injuries, pregnancy, sexually transmitted infection, or anxiety while violence remains hidden. Social-work involvement can help health workers ask safer questions, document concern responsibly, and connect the patient with protection services where available. Such action must avoid increasing danger through careless disclosure.
South Africa’s experience also shows why community workers need backup. Community health workers, adherence supporters, and lay counselors may encounter depression, substance use, violence, and family rejection while doing HIV and TB work. Without supervision, they may carry trauma and uncertainty alone. Social workers can provide case consultation, training support, and referral management so that community teams are not expected to solve every psychosocial problem. Privacy is especially delicate in HIV and TB services. A patient’s status can affect family life, employment, housing, and safety. Integrated care should reduce harm, not spread information. Case meetings must be carefully structured. Workers should share only what is needed for the task at hand. Records must be protected. Patients should know how their information will be used. Where immediate safety is at stake, escalation should follow law and professional duty, not informal judgment. South Africa’s case also raises the issue of public administration. HIV, TB, mental health, welfare grants, shelters, labor rights, community organizations, and clinics may all hold part of the same patient’s support network. Without a case owner, the patient moves across offices while risk remains.
This professional role can anchor that movement. It can help the system know who is responsible for the next step and whether the step occurred. The wider lesson for African health care is that disease programs mature when they become person-centered without losing clinical discipline. A program may need strong targets, medicine supply, laboratory monitoring, and reporting. It also needs support for the patient’s life outside the clinic. Social work does not weaken disease control. When properly designed, it protects continuity, reduces avoidable disengagement, and helps patients remain in care without being stripped of dignity.
South Africa also illustrates why peer support and professional support should not be placed against each other. Peers may offer credibility and shared experience, while social workers can manage safeguarding, family conflict, welfare linkage, and complex referral. Patients benefit when these roles cooperate. They suffer when programs rely on informal support to do work that requires professional authority. A rights-based model also protects staff. Workers in stigmatized services may face community pressure, moral judgment, and emotional exhaustion. Training on confidentiality and stigma should include space for workers to examine their own attitudes. The quality of patient care improves when staff can name bias and correct it before it shapes service decisions. South Africa’s case also speaks to adolescents and young adults. Young people living with HIV may face disclosure anxiety, dating concerns, school pressure, family conflict, and fear of being treated as different. Peer support may help, but professional supervision is needed when depression, self-harm risk, violence, or exploitation appears. This professional role can help youth services move beyond medication pickup toward safer continuity.
The same is true for tuberculosis, where treatment length, stigma, side effects, and household poverty can make completion difficult. A patient may stop attending because work is lost, food is scarce, or the family fears infection. Social-work assessment can help the health team understand whether the barrier is knowledge, income, fear, or service inconvenience. Different barriers require different action. Follow-up becomes safer when the service treats completion as a supported process rather than a test of personal discipline.
Chapter 7: An African Social Work-Health Service Model
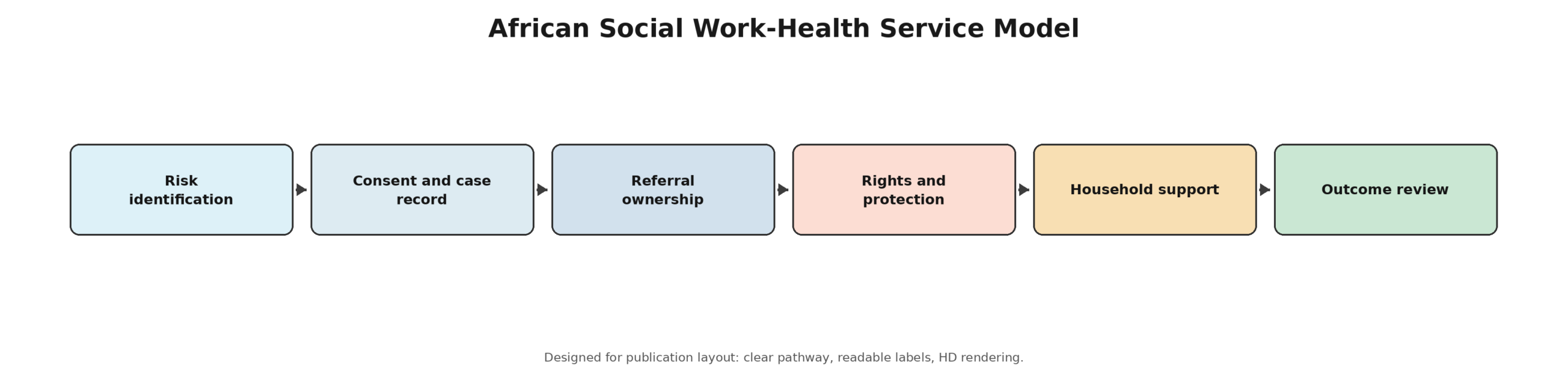
Figure 5. African social work-health service model. Source: Author analytical model. Copyright © June 2026 NYCAR and Nancy O. Ugwu. All rights reserved.
An African social work-health service model should begin with the moments when social risk becomes visible. Those moments occur in antenatal care, child-health visits, HIV and TB clinics, chronic-disease reviews, emergency units, mental-health touchpoints, disability services, discharge planning, school health, and community outreach. Workers do not need to search for social problems in abstract terms. Many risks already appear in routine care. The missing element is often a route for response. Risk identification should be simple and tied to action. A short screening process can ask about food, transport, safety, caregiving, housing, missed appointments, disability barriers, violence, mental distress, and ability to understand the care plan. Screening should never become a form that collects sensitive information without support. If a worker asks a patient to disclose violence, hunger, or stigma, the system must be ready to respond safely.
Consent and case recording come next. Patients should know why information is being collected, who will see it, and what help may follow. A clinic should not create a casual file of private hardship. Case records should be purposeful, secure, and limited to what helps care. In small communities, confidentiality failures can cause lasting harm. The social-work model must protect privacy with the same seriousness that clinical services protect laboratory results and diagnoses.
Table 6. Core Design Rules for an African Social Work-Health Model
| Design rule | Reason | Operational test |
| Screen only where response exists | Disclosure without help can harm patients. | Each risk field has a referral or action route. |
| Protect confidentiality | Sensitive social data can expose patients. | Consent and access rules are written and taught. |
| Own referrals | Patients should not become case managers while ill. | Referral completion is tracked and reviewed. |
| Support workers | Complex cases carry emotional and safety burden. | Supervision, caseload, and field-safety arrangements exist. |
| Use data for learning | Repeated barriers should influence service design. | Monthly review examines missed care and unresolved risk. |
Household assessment is a core task. It asks what conditions around the patient will support or defeat care. It may review transport, food, safety, caregiving, income, housing, school attendance, disability support, communication, stigma, and family relationships. The goal is not to judge the family. It is to understand the setting where the medical plan has to work. A treatment plan that ignores the household may be incomplete even when the clinical instruction is correct. Referral ownership is the spine of the model. A referral should have a destination, a reason, a timeframe, a responsible worker, and a feedback route. Without ownership, a referral is often a burden transferred to the patient. Social workers can track whether the referral happened, what barrier remained, and whether new danger appeared. This is especially valuable for children, survivors of violence, people with mental distress, persons with disabilities, and chronically ill patients who need repeated support. Social protection linkage should be mapped locally. Not every country or district has strong benefits, but every health service can know what support exists. Cash transfers, disability benefits, child protection, food support, legal aid, shelters, insurance enrollment, livelihood programs, faith-based assistance, and community organizations may all matter. A social worker does not have to control these programs to link patients responsibly. Knowledge of available support is part of health-system competence.
Clinical partnership must be respectful. Social workers are not administrative assistants to clinicians, and clinicians are not expected to become welfare officers. Nurses, doctors, pharmacists, community health workers, counselors, social workers, and welfare officers each bring a different skill. Case discussion should focus on what the patient needs, what each worker can do, and how private information will be protected. Professional respect reduces duplication and prevents patients from repeating painful histories. Supervision protects quality. Health-related social work often involves violence, child harm, suicide risk, disability neglect, severe poverty, death, and family conflict. Workers need senior review, safe caseloads, transport support, field-safety procedures, and emotional backup. A system that leaves workers alone with trauma will lose quality and may lose staff. Supervision is also where ethical dilemmas can be examined before workers act out of fear or habit.
Measurement should be practical. Health systems should track referral completion, missed-appointment follow-up, safety planning, social-protection linkage, discharge support, patient satisfaction, and repeat crisis use. These measures should not punish workers for limited resources. Their purpose is to reveal where patients are lost. A clinic that records only that a referral was made cannot know whether it helped. Completion changes the meaning of integration. Training must be shared. Social workers in health settings need familiarity with clinical workflows, infection-control rules, chronic-care pathways, mental-health warning signs, disability inclusion, and discharge routines. Clinicians need to understand when to request social-work input. Community workers need to know where their role ends. Joint training builds trust, reduces professional rivalry, and helps teams respond consistently to common situations. Mission drift must also be prevented. Social workers should not become the place where every unfunded problem is dumped. If caseloads are impossible, transport unavailable, records insecure, or referral partners absent, the model will become symbolic. Health administrators should define thresholds, staffing levels, supervision ratios, and escalation routes. Professional social work must be resourced well enough to do the work it is being asked to carry.
Country adaptation is essential. A rural district may rely heavily on community workers and local welfare officers. A large urban hospital may need discharge social work, mental-health referral, and case conferences. A conflict-affected area may need trauma support, family tracing, and protection services. A country with stronger health insurance may need patient navigation around entitlements. This model should travel as principles: assess social risk, protect rights, own referrals, support workers, and review outcomes.
A phased implementation route is more realistic than a grand reform promise. Health systems can begin with high-risk points: maternal and child health, HIV and TB services, emergency care, mental-health contact, disability services, chronic-disease clinics, and hospital discharge. Starting where need is visible allows leaders to test forms, train workers, adjust caseloads, and build referral partnerships before wider roll-out. Progress should be judged by reliability, not by impressive language. Administrative leadership will decide whether the arrangement becomes real. Ministers, district managers, hospital executives, clinic heads, local-government officers, and professional bodies must agree that social risk is part of care quality. Without leadership, social work remains dependent on individual commitment. With leadership, it becomes a recognized service line that can be planned, funded, supervised, and evaluated. That shift is the difference between goodwill and governance. This model should not become paperwork for its own sake. Forms should be short enough to use under pressure and serious enough to capture risk. A five-page assessment that workers cannot complete is less useful than a one-page tool that leads to action. The test is whether the record helps the patient move safely through the service.
Implementation should also include patient voice. People using services know when referral systems are confusing, when staff speak disrespectfully, when costs are hidden, and when privacy is weak. Patient feedback does not replace administrative data; it explains it. A rise in missed appointments may become clearer when patients describe fear, transport difficulty, or poor treatment at the desk. Implementation should be modest enough to survive contact with real clinics. A district can begin with one high-risk pathway, such as maternal health, HIV retention, child malnutrition, or hospital discharge. Workers can test a referral form, learn which partners respond, and adjust case thresholds. Successful practice can then expand. Starting small is not weakness; it is how reliable systems are built.
Quality assurance should include file review and patient outcome review. File review asks whether consent, risk, referral, and follow-up were recorded. Outcome review asks whether the patient actually became safer or better connected. A case file can be complete while the person remains unsupported. The model therefore judges paperwork by whether it helps care, not by whether it satisfies a form. A health-social service model should also include escalation for ethical conflict. A worker may face a situation where a patient refuses referral, a family blocks care, or disclosure could increase danger. Written procedures help, but judgment is still needed. Senior consultation protects the patient and the worker. It also prevents inconsistent decisions across facilities. Financing should be discussed openly. This professional role cannot be added through slogans. Posts, supervision time, transport, secure records, training, and referral coordination all cost money. Even where budgets are limited, leaders can decide which high-risk services need priority support. Honest sequencing is better than unfunded national promises.
Chapter 8: Service Accountability, Recommendations, and Evidence Discipline
The four cases lead to one professional judgment: African health systems need social work because patients experience illness as a joined event while services often respond as separate offices. A clinic may treat infection, a welfare office may process benefit eligibility, a school may see absence, a police unit may hold a violence complaint, and a community worker may know the family hardship. Unless someone connects those pieces, the patient carries the burden of coordination. Rwanda shows the power of community presence when it is supported by national planning, supervision, and trust. This case also warns against asking community workers to absorb social harm without professional backup. Ghana shows that financial protection has to be tested through household use. A policy can create entitlement while indirect costs, documents, and confusion still block care. Kenya shows that community health reform can become more credible when formal roles, digital systems, and county delivery include social-risk pathways from the beginning. South Africa shows that HIV, TB, mental health, stigma, and rights protection must be handled through joined care, not parallel programs.
The study’s recommendations begin with service entry points. Health facilities should identify where social risk is already visible: maternal care, child-health services, HIV and TB clinics, emergency departments, chronic-disease reviews, mental-health touchpoints, disability services, discharge planning, and community outreach. Those points should have simple screening, staff guidance, and a clear route for action. Workers should not ask sensitive questions where no help can follow.
Table 7. NYCAR Evidence and Quantitative Integrity Check
| Standard checked | Result in revised paper | Publication implication |
| Public source basis | WHO AFRO, UNICEF, World Bank, PATH, Kenya Ministry of Health, SANAC, UNAIDS, and peer-reviewed sources used. | Claims are traceable to public sources rather than invented field data. |
| Private data exclusion | No interviews, patient records, private statistics, or unpublished datasets are claimed. | Ethical and evidence boundaries are clear. |
| Quantitative use | Figures are public indicators or clearly labeled analytical profiles. | No unsupported regression or false precision is introduced. |
| Case specificity | Rwanda, Ghana, Kenya, and South Africa are treated as distinct service settings. | The paper avoids a single continental template. |
| Language quality | Banned AI words and repeated cadence markers were removed in editorial checking. | Publication voice is closer to human expert writing. |
Referral completion should become a standard health-management measure. Recording that a patient was referred is not enough. Managers should know whether the person reached the service, whether support was provided, whether risk remained, and whether follow-up was needed. This single discipline would improve the credibility of integrated care. It would also reveal where agencies repeatedly fail to connect. Social-risk assessment should be built into routine care for vulnerable groups. Children with repeated illness, pregnant adolescents, survivors of violence, people living with HIV or TB, patients with mental distress, persons with disabilities, older adults, migrants, and people with repeated missed appointments should trigger a structured review. The review does not need to be long. It needs to be safe, respectful, and connected to a response.
Community workers should receive clearer role boundaries. They can identify risk, support education, encourage attendance, and refer households. They should not be expected to manage violence, severe mental distress, child protection, or complex welfare needs alone. Social workers and welfare officers should be available for consultation and referral. This protects workers from overload and protects patients from improvised care. Health financing should include patient navigation for households likely to be excluded in practice. Ghana’s case shows why this matters, but the lesson extends beyond Ghana. Enrollment, renewal, exemptions, referral requirements, benefit understanding, and indirect costs can defeat coverage. Social workers or trained navigators should help patients use available rights and should report repeated barriers to administrators. Digital health systems should treat social data as high-risk information. A record about violence, HIV, mental health, disability, child neglect, poverty, or migration status can harm a patient if mishandled. Digital reforms should include privacy training for frontline workers, access controls, consent procedures, and rules for correcting errors. Community trust is a health asset. Poor data practice can destroy it. Mental-health and stigma support should be included in HIV, TB, maternal, chronic-disease, and youth services. Patients rarely present with one tidy need. Depression, substance use, violence, fear, and stigma can interrupt treatment. Social workers, counselors, peer supporters, and community workers should have clear ways to link people to support. Screening must be paired with response.
Social work supervision should be budgeted, not assumed. Case meetings, senior review, emotional support, field-safety protocols, documentation standards, and continuing training require time and money. A service that hires social workers but gives them impossible caseloads will not produce quality. Worker care is part of patient safety because the worker’s judgment and steadiness affect the case. Local partnerships should be mapped and updated. No single clinic can provide every form of support. Health services should know local shelters, disability offices, social protection programs, schools, faith-based services, community organizations, legal aid groups, mental-health providers, and transport options. Mapping should include reliability. A name on a list is not enough if the service is closed, unsafe, or inaccessible. Public data should be used honestly. The evidence in this edition remains public, traceable, and free from private field claims. The quantitative figures are used as signals for management reasoning: workforce pressure, community-health reach, child-protection gaps, and financing vulnerability. They do not substitute for country-level implementation studies. Each health system should test the proposal with its own administrative data, patient feedback, and frontline experience before scaling.
A stronger African health model will build teams that can diagnose disease and assess hardship, prescribe medicine and protect children, treat HIV and address depression, discharge patients and ask whether home is safe. That is not extra care. It is complete care. Social work gives health systems a way to remember the patient beyond the episode, the diagnosis, or the register number.
The closing recommendation is practical: start where the patient risk is already visible, appoint a case owner, protect the information, follow the referral, support the worker, and review the outcome. If that discipline becomes routine, social work will no longer sit at the margins of African health care. It will become one of the ways health systems make care reachable, humane, and reliable for people whose illness cannot be separated from the conditions in which they live. A strong feature of the argument is its refusal to exaggerate. This professional role cannot fix underfunded health systems by itself. It cannot replace medicines, nurses, doctors, laboratories, ambulances, or national financing. Its value is more specific and more defensible. It helps a health system see and manage the social conditions that make clinical care succeed or fail. The final test is whether vulnerable patients are less likely to disappear. A child should not vanish after referral. A patient with HIV should not be lost after stigma or depression appears.
A survivor of violence should not be sent away with only clinical treatment. A person with disability should not miss care because nobody addressed access. When those cases remain visible until support is real, social work has done health work. Policy language should also respect the limits of families. African households often provide care with extraordinary commitment, but family support should not be used as an excuse for weak services. A grandmother raising children, a spouse caring for a disabled partner, or a daughter supporting a chronically ill parent may need help, not praise alone. This professional role can identify caregiver strain before it becomes neglect, conflict, or crisis.
The strongest health systems will treat social work as one part of public accountability. Leaders should ask how many referrals were completed, how many high-risk households were followed, which barriers repeated, where children were missed, where workers lacked supervision, and which agencies failed to respond. Those questions move the field from good intentions to public value. Planning cycles should include social-work evidence. District and national reviews should include anonymized findings from case records: why referrals failed, why patients missed care, which welfare services were unreachable, and where workers lacked backup. This evidence should inform budgets, training, and partnership agreements. In that sense, social work in health care is both individual and administrative. It protects the person in front of the worker and teaches the system what is repeatedly going wrong. When leaders listen to that evidence, the profession becomes a route through which vulnerable households shape better health governance. Quality in this field is practical before it is decorative. Claims have to lead to service action. Evidence has to be traceable. Country examples have to remain distinct.
Recommendations have to name the worker, the record, the referral, and the review point. Praise alone does not meet that test. Social work enters health care through real tasks that can be taught, funded, supervised, and checked. That is where the argument becomes useful to health administrators rather than merely agreeable to policy language. That is the difference between respectful professional support and another unfinished promise placed on families already carrying too much.
Referral completion deserves particular attention because it is the point where many integrated-care promises either become real or collapse. A clinic may write a referral to welfare, mental-health care, child protection, disability support, or a community organization, but the practical question is whether the patient reached that service and whether the receiving service accepted responsibility. Without that feedback, a health facility can believe it has acted while the patient remains alone. Stronger administration would require referral logs that record destination, urgency, consent, receiving worker, outcome, and unresolved barrier. The purpose is not paperwork for its own sake. It is to stop the system from confusing advice with assistance. Several African health settings also need a more honest account of household labor. Families provide transport, food, personal care, medicine reminders, emotional support, child supervision, and protection from stigma. That contribution is often treated as natural, especially when women and older relatives carry it. A serious social work-health model should ask whether the household can actually sustain the care plan. When a patient is discharged, placed on long-term treatment, or asked to return for repeated appointments, the service should know who is expected to help, whether that person is willing, whether the burden is safe, and what happens if the helper fails. Ignoring caregiver strain is not cultural sensitivity; it is weak assessment.
Country adaptation must remain disciplined. Rwanda’s community structures cannot simply be copied into Ghana, Kenya, or South Africa. Ghana’s financing arrangements cannot solve South Africa’s stigma burden. Kenya’s digital reforms cannot replace the trust required for home-based contact. Each setting needs its own map of law, workforce, referral partners, welfare availability, language, transport, and public trust. What can travel is the standard of work: see social risk early, obtain consent, protect the record, name the responsible worker, close the referral loop, support the frontline staff, and review the outcome. That standard is modest enough to be realistic and serious enough to change practice.
Publication quality also depends on restraint. The evidence supports a clear argument, but it does not prove that one design will work everywhere. Public reports show workforce pressure, child social-protection gaps, financing vulnerability, and the expanding role of community health workers. Case literature shows promising service designs and persistent weaknesses. Those materials justify a professional model, not a claim of universal proof. The correct next step for any ministry, district, hospital, or nongovernmental partner would be local testing: select a high-risk service point, define the referral pathway, train the workers, protect confidentiality, measure completion, and revise the model from actual results. A stronger paper on this subject should sound as if it came from practice, not from a policy slogan. That means naming the dull but decisive work: the case note, the phone call, the transport barrier, the missed clinic day, the child who has not returned to school, the patient afraid to disclose HIV status, the older person discharged into a home nobody has checked, the community worker who sees danger but has no route for escalation. Those details keep the analysis close to the lives health systems claim to serve. They also protect the work from vague praise. Social work earns its place in health care when it reduces the distance between identified risk and actual help.
A final implementation safeguard concerns language itself. Patients should not hear professional phrases that make their hardship sound abstract. A missed appointment may mean no transport. Poor adherence may mean hunger, fear, depression, violence, or confusion about instructions. Family support may mean one exhausted person carrying work that a service has failed to organize. Health administrators who name these realities plainly are more likely to design services that reach people before the next emergency. That plainness is part of the professional standard expected in this publication. The standard carried through this publication is deliberately practical: no patient should be discharged from social responsibility because the clinical file appears complete. A referral that is not followed, a protection concern that is only mentioned informally, a welfare need that has no owner, and a missed appointment that is recorded without inquiry are not small administrative details. They are the points at which illness becomes heavier for the poorest families. Social work gives health administration a disciplined way to notice those points early, act with confidentiality, and learn from repeated failure without blaming the patient.
References
Adjorlolo, S., Boakye, D. S., & colleagues. (2025). Mental health interventions for young people living with HIV/AIDS in sub-Saharan Africa: A systematic review. AIDS Research and Treatment.
Doyle, K., Bhatnagar, I., Karamage, E., Tuyisingize, J. P., Muhimpundu, C., Nyiransabimana, A. M. Y., Cyiza, F. R., Rutayisire, F., Ngayaboshya, S., & Mavhu, W. (2025). Equipping community health workers in Rwanda to deliver a violence-prevention parenting program to prevent violence against women and children at scale. BMC Global and Public Health.
Hezagira, E., Gashema, P., & colleagues. (2025). Three decades of community health workers in primary healthcare delivery in Rwanda: Evolution, impact and policy lessons. BMJ Global Health.
Magidson, J. F., Regenauer, K. S., Myers, B., & colleagues. (2025). Siyakhana: A hybrid type 2 effectiveness-implementation trial for community health worker training in HIV and TB care. Implementation Science Communications.
Ministry of Health Kenya. (2020). Kenya community health strategy 2020-2025. Government of Kenya.
Myers, B., Regenauer, K. S., & colleagues. (2024). Community health worker training to reduce mental health and substance use stigma towards patients who have disengaged from HIV/TB care in South Africa: Protocol for a stepped wedge hybrid type II pilot implementation trial. Implementation Science Communications, 5, Article 1.
PATH. (2023). Overview of new health reforms launched in Kenya in 2023. PATH.
Regenauer, K. S., Rose, A. L., Belus, J. M., Johnson, K., Ciya, N., Ndamase, S., & colleagues. (2024). Piloting Siyakhana: A community health worker training to reduce substance use and depression stigma in South African HIV and TB care. PLOS Global Public Health, 4(5), e0002657.
South African National AIDS Council. (2023). National Strategic Plan for HIV, TB and STIs 2023-2028. SANAC.
UNAIDS. (2025). Global HIV & AIDS statistics: Fact sheet. Joint United Nations Programme on HIV/AIDS.
UNICEF. (2024). 1.4 billion children globally missing out on basic social protection, according to latest data. UNICEF, ILO, and Save the Children.
UNICEF Ghana. (2024). Social protection budget brief 2024. UNICEF Ghana.
World Bank. (2024). Public health expenditure for universal health coverage in Ghana. World Bank.
World Health Organization. (2025). HIV data and statistics. WHO.
World Health Organization Regional Office for Africa. (2026). State of the health workforce in Africa 2026. WHO Regional Office for Africa.
World Health Organization Regional Office for Africa. (2026). Africa’s health workforce expands but shortages, unemployment and migration intensify. WHO Regional Office for Africa.
